William C. Hsiao, Ph.D.
NEJM, March 16, 2011
The United States faces two major problems in the health care arena: the swelling ranks of the uninsured and soaring costs. The Patient Protection and Affordable Care Act (ACA) makes great strides in addressing the former problem but offers only modest pilot efforts to address the latter. Experience in countries such as Taiwan and Canada shows that single-payer health care systems can achieve universal coverage and control inflation of health care costs. Because of strong political opposition, however, the U.S. Congress never seriously considered a single-payer approach during the recent reform debate. Now Vermont, wishing to solve the intertwined problems of costs and access through systemic reform, is turning in that direction. Vermont Governor Peter Shumlin campaigned on a platform of single-payer health care, and Democratic legislative leaders are committed to this approach.
In Vermont, the status quo in health care has become untenable. Despite numerous reforms over the past 15 years, Vermont’s health care costs are escalating rapidly, straining the state budget, household incomes, and employers’ bottom lines. More than 7% of Vermonters are uninsured, and another 15% have inadequate insurance.
The Vermont Legislature passed Act 128 in May 2010 authorizing a study to find the most viable and practical systemic solutions to these problems.1 The goals are clear and ambitious: Vermont wants to achieve universal coverage, reduce the rate of cost increases, and create a primary care–focused, integrated delivery system. The question is how to achieve those goals. My team of health system analysts at the Harvard School of Public Health was commissioned by the Vermont Legislature to develop and evaluate three options for health system reform and determine which option would best achieve the stated goals.
We conducted extensive fiscal, legal, institutional, and stakeholder analyses in Vermont to gain an in-depth understanding of the hurdles confronting any such plan and to design ways of overcoming or navigating around them. Our findings presented a striking picture. Vermont faces a $150 million budget shortfall. Employers argue that health care costs jeopardize their businesses’ financial viability, while families struggle to pay out-of-pocket health care costs. Vermont businesses and workers are unwilling to spend more for health care.
On the other hand, Vermonters are also largely unwilling to reduce their level of benefits. Our analysis found that, on average, Vermonters have rich insurance benefits approaching the ACA’s “platinum” standard. Similarly, physicians and hospitals are unwilling to accept reductions in their net incomes.
Our analyses led us to adopt several design principles that shaped our recommended design. First, we wanted to design a system capable of achieving universal coverage and reducing the cost inflation rate. Any increases in spending to cover the uninsured and underinsured would have to come from savings generated by systemic reforms. Any financing mechanism should not increase the costs to the state, businesses, and households. Second, we aimed to maintain Vermonters’ current average benefits. Third, we sought to maximize federal revenues from all sources. Fourth, we would not reduce overall net income of physicians, hospitals, or other providers. Finally, we sought to eliminate the perverse incentives inherent in the fee-for-service system, through risk-adjusted capitation payment plus performance bonuses, to provide incentives for the formation of accountable care organizations and care integration.
We found that the system capable of producing the greatest potential savings and achieving universal coverage was a single-payer system — one insurance fund that covers everyone with a standard benefit package, paying uniform rates to all providers through a single payment mechanism and claims-processing system. Our analysis showed that Vermont could quickly save almost 8% in health care expenditures through administrative simplification and consolidation, plus another 5% by reducing fraud and abuse.
We recommended that the single payer be a public–private partnership. An independent board with representation from both the major health care payers (employers, the state, and workers) and the major beneficiaries and recipients of payment (providers and consumers) would negotiate updates to the benefit package and payment rates. We also proposed contracting out claims administration through a competitive bid to create incentives to develop more efficient systems.
This system reduces the rate of cost increases over time by insulating major decisions about health care spending from politics, as well as by paying providers through capitation rather than fee for service, promoting delivery-system integration, and reducing the practice of defensive medicine by implementing a no-fault medical malpractice system. All told, we estimated that Vermont could save 25% in health care expenditures over 10 years (estimated savings for the first 5 years are shown in the table).
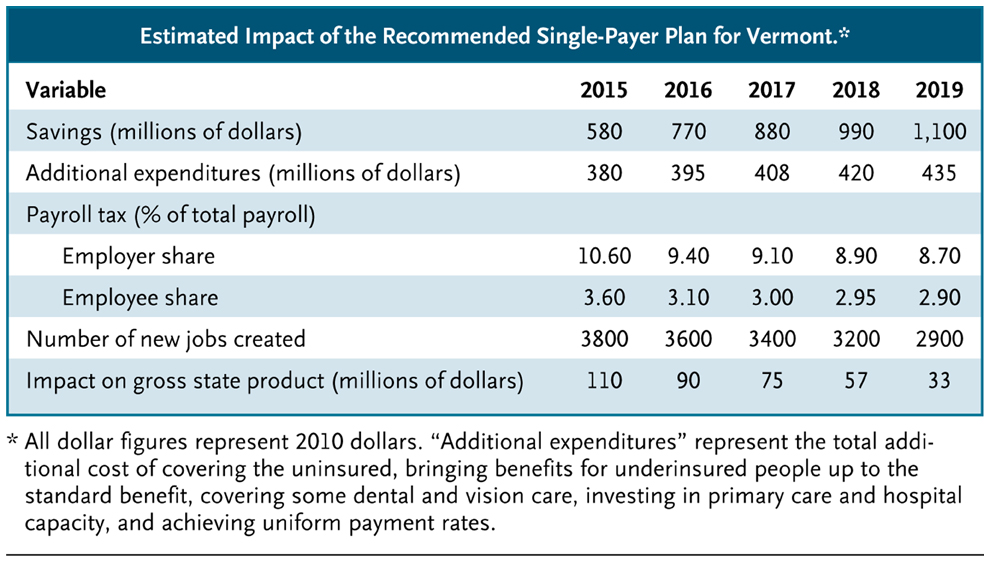
Estimated Impact of the Recommended Single-Payer Plan for Vermont.
Eligibility for coverage in the system would be based solely on proof of Vermont residency, the same requirement currently used by Vermont Medicaid; this approach effectively divorces health benefits from employment. However, we proposed to finance the system through a payroll contribution on all Vermont wages, split between employer and employee, to preserve the federal tax treatment of health benefits — a tax expenditure worth $400 million to $500 million in Vermont. We recommended delaying the implementation of the single-payer system until after Vermont’s insurance exchange has been operating for a year, at which point the state will have a basis for arguing for a waiver from the ACA requirements and estimating the amount of a federal block grant it would receive before 2017, when current ACA law allows for waivers.1
We used two economic models to estimate the impact of the proposed system. We fed estimated savings and costs under the single-payer system into a MicroSimulation Model, developed by the Massachusetts Institute of Technology’s Jonathan Gruber, which simulated the likely responses to the ACA by employers and low-income workers and estimated the amount of state and federal spending under the law, as well as computing the payroll contribution rates necessary to finance our plan. We then fed those results into a macroeconomic model developed by Regional Economic Models to estimate the effects on jobs and the gross state product that would result from additional spending for health care when more people were covered and the increase in household income and consumption when insurance premiums decreased with a single-payer plan. The models predicted that, as compared with implementing the ACA, the single-payer system would result in lower spending by employers, the state, and households and in the creation of more jobs in Vermont. For example, without single-payer reforms, we predict that employers would pay 12% of their payrolls in health insurance premiums in the first year, with further increases to follow.
The governor has already introduced legislation establishing the first building blocks of a single-payer system: payment reform, the creation of the independent board, and the mandate to build Vermont’s health insurance exchange as a platform for a single-payer infrastructure. Legislation establishing universal coverage and its
financing will follow, when the state can obtain waivers from Medicare’s and Medicaid’s provider-payment rules and the ACA’s individual mandate and subsidy rules. Innovative state reforms are being encouraged, as illustrated by President Obama’s support for the Wyden–Brown bill,2 which would grant waivers from ACA requirements in 2014 if states can meet the ACA’s goals. The Vermont single-payer plan certainly can.
Perhaps we are at the dawn of systemic reform in U.S. health care. The Vermont single-payer plan will never be as efficient as Taiwan’s or Canada’s because it must work within the bounds of federal laws and programs and the realities of porous state borders. Nevertheless, it can produce substantial savings to fully fund universal coverage, reduce health care costs for most businesses and households over time, and reform a fragmented delivery system. Of course, someone will bear the burden — mostly the private insurance industry and high-wage businesses that don’t currently offer insurance. But if Vermont can navigate its political waters and successfully implement this plan, it will provide a model for other states and the country as a whole.
Disclosure forms provided by the author are available with the full text of this article at NEJM.org.
This article (10.1056/NEJMp1100972) was published on March 16, 2011, at NEJM.org.
Source Information
From the Department of Health Policy and Management, Harvard School of Public Health, Boston.
References
1. Act 128 Health System Reform Design Final Report. (http://www.leg.state.vt.us/jfo/healthcare/FINAL%20REPORT%20Hsiao%20Final%20Report%20-%2017%20February%202011_3.pdf.)
2. Stolberg SG, Sack K. Obama backs easing state health law mandates. New York Times. February 28, 2011.