Auditing Access to Specialty Care for Children with Public Insurance
By Joanna Bisgaier, M.S.W., and Karin V. Rhodes, M.D.
The New England Journal of Medicine, June 15, 2011Expansions of Medicaid and the Children’s Health Insurance Program (CHIP) are designed to extend access to high-quality medical care to all U.S. children. However, evidence suggests that the 37 million children covered by Medicaid–CHIP are less likely to receive specialty care than children covered by commercial insurance.
We designed an audit study in which research assistants posing as mothers made paired calls to the same clinic and attempted to schedule an appointment for a child needing specialty care. The calls were separated by 1 month and varied only by insurance status (private vs. Medicaid–CHIP insurance).
With the use of an experimental study design involving simulated requests for specialty care, we measured real-world scheduling behavior in an urban area with a high density of medical specialists. The results showed significant disparities in children’s access to needed outpatient specialty care, attributable to specialists’ reluctance to accept public health insurance. These results held across all audited specialties. (66% of the callers reporting Medicaid–CHIP coverage were denied an appointment for specialty care, as compared with 11% of the callers reporting Blue Cross Blue Shield insurance.) Moreover, even when children with Medicaid–CHIP were not denied appointments outright, the appointments were, on average, 22 days later than those obtained for privately insured children with identical health conditions (even though the clinical scenarios represented urgent situations).
Overall, we found considerable disparities in access to outpatient pediatric specialty care that were attributable to providers’ nonacceptance of public insurance.
A well functioning health care system removes barriers to the care that patients need. It is sad commentary that the United States has a program for the most needy that instead crates a barrier to care. As this study shows, merely being covered by Medicaid disqualifies many children from being able to access the specialized care that they need.
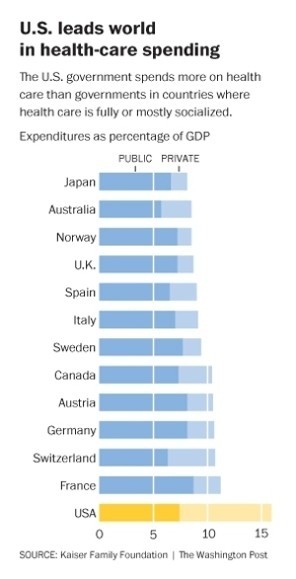
This doesn’t happen in other nations. If a person needs care, access is automatically provided without any thought given to the mechanism of payment.
In the United States, even though we have more than enough money already in the system to pay for all essential care, we have erected a wasteful, fragmented, dysfunctional financing system that creates barriers that must be negotiated before appropriate care can be obtained. It’s not the money; it’s the flawed financing system.
We need to cast aside these barriers and create an equitable financing system that is automatic – a single payer national health program. We have the money. Now all we need is the political will.