Our Commitment to Help Those Who Have Too Little
President Franklin Delano Roosevelt said that progress is helping those in need. President Donald Trump by words and actions advocates for the wealthy. Today’s progressives are enthusiastically received when advocating for helping everyone, yet the Democratic party often favors the wealthy. We must commit to helping those in need via programs that support us all.
Second Inaugural Address of Franklin D. Roosevelt, January 20, 1937
The test of our progress is not whether we add more to the abundance of those who have much; it is whether we provide enough for those who have too little.
Second Inaugural Address of Donald Trump, January 20, 2025
Instead of taxing our citizens to enrich other countries, we will tariff and tax foreign countries to enrich our citizens.
We will restore the name of the great president William McKinley to Mount McKinley, where it should be and where it belongs. President McKinley made our country very rich through tariffs and through talent. He was a natural businessman.
The Democratic Party Faces a Voter Registration Crises, The New York Times, August 20, 2025, by Shane Goldmacher with Jonah Smith
Of the thirty states that track voter registration by political party, Democrats lost ground to Republicans in every single one between the 2020 and 2024 elections – and often by a lot. That four-year swing toward Republicans adds up to 4.5 million voters, a deep political hole that could take years for Democrats to climb out from.
Comment:
By Don McCanne, M.D.
Since I was a small child, I always believed in the principle that my father taught me that was so well expressed by President Roosevelt: we always take care of each other.
Currently we are operating under a principle expressed by President Trump: we strive to further enhance the wealth of those who have much, while taking away from those who have little.
This contrast in principles correlates with the respective political parties of Presidents Roosevelt and Trump. Yet, we now see a shift wherein the Democrats seem to be joining the Republicans in placing more value on personal wealth than they do in supporting a government that would ensure that those who have too little would be adequately cared for.
How can this be when polls show majority support for social programs such as single payer Medicare for All? Rallies, such as those of Bernie Sanders and AOC, have record-breaking attendance when they promote programs that would enable all of us to meet basic needs in life. And the Republicans who hold town hall forums in their districts are met with boos and catcalls when they boast about laws they supported that would enhance the wealthy while ignoring the needs of those who are struggling.
Where should our loyalty stand? Should it be in support of social justice which takes care of everyone – including those who have too little? Or should it be for personal wealth creation that benefits only the most affluent amongst us? I certainly have my answer to these questions, and I fail to see why a majority of us would choose the other answer. Votes should not blindly follow arbitrary loyalty to a political party. They should be based on respect we have toward fellow humans.
If someone can present me with a moral argument of why I might be wrong, I would certainly like to hear it, though I am prepared to counter any such argument. I will never accept that personal wealth is more important than our individual and collective souls.
https://healthjusticemonitor.org…
Stay informed! Subscribe to the McCanne Health Justice Monitor to receive regular policy updates via email, and be sure to follow them on Twitter @HealthJustMon.
Trump’s Big Bill Will Make It Harder for Doctors to Give Patients the Care They Need
Work requirements for Medicaid don’t encourage employment; they punish illness and make recovery harder.
By Hridaya Shah and Toby Terwilliger, M.D.
Common Dreams, Aug. 22, 2025
Like most bright-eyed medical students entering the wards for the first time, I was eager to give my patients the best that modern medicine could offer. This is far from the reality that I was confronted with—one’s insurance status dictated care as much as any guideline, evidence, or well-intentioned physician ever could.
I cared for patients whose chronic illnesses forced them to stop working, only to be told that without a job, they no longer qualified for Medicaid. The logic is cruelly circular: Lose your health, lose your job, lose your care. Work requirements for Medicaid don’t encourage employment; they punish illness and make recovery harder.
Alongside countless peers and healthcare professionals, I was incredibly disheartened on July 4, 2025 as I watched US President Donald Trump sign into law the most sweeping healthcare overhaul since the Affordable Care Act. The 870-page One Big Beautiful Bill Act (OBBBA) is projected to strip health coverage from 11.8 million Americans, leading to an estimated 24,000 preventable deaths each year—driven largely by drastic changes to Medicaid’s administration.
The current administration has long touted work requirements as a fix to Medicaid, having approved 13 Medicaid Section 1115 demonstrations with work requirements in its first term. Unfortunately, it has ignored the failures of these waiver programs and doubled down, making ineffective work requirements the law of the land.
The Majority of Medicaid Recipients Are Already Working
President Trump and his administration have repeatedly stated that the integrity of the Medicaid program needs to be restored, promoting narratives of Medicaid waste, fraud, and abuse. As such, work requirements for “able-bodied” Medicaid recipients were a key provision in the OBBBA. However, in reality, 92% of Medicaid beneficiaries are already working, caring for family, attending school, or living with a disability. Only 8% are “able-bodied” adults not seeking employment.
States Have Tried Work Requirements, They Don’t Work
Arkansas was the only state to have a statewide Medicaid work requirement waiver approved. The results were catastrophic; over 18,000 beneficiaries lost coverage in the four months before a judge ruled that the program could not continue. While enacted, the waiver failed to increase employment; instead implementation was associated with increased Medicaid churn, medical debt, and loss of health coverage.
For other states, like Michigan and New Hampshire, the path to work requirements was mired with legal challenges. Both states proposed work requirements, which would have resulted in nearly 80,000 and 17,000 beneficiaries losing coverage, respectively, had the programs not been suspended before taking effect.
As of July 2025, Georgia is the only state with active work requirements through the Pathways to Coverage program. Results of this program are similarly underwhelming, with only 8,000 enrolled as of June 2025 after two years of rollout and millions spent in administrative costs. Enrollment falls far short of the projected 64,000 enrollees or the 300,000 to 400,000 Georgians who would qualify for coverage under full Medicaid expansion.
The OBBBA Doubles Down on Failed Policy
The OBBBA will require all states to follow Georgia’s path by 2027. Based on Congressional Budget Office (CBO) estimates, the federal government will save $900 billion in Medicaid spending over the next decade, with work requirements accounting for a third of the reduced spending. These savings come at an enormous cost—approximately 5 million individuals are projected to lose access to Medicaid by 2034, 1.22 million jobs in the healthcare sector will vanish in the next decade, and unemployment will rise by 0.8%. The consequences of this bill will be devastating.
Medicaid Expansion is a Job Promotion Program
Overwhelming evidence suggests Medicaid expansion has reduced uninsurance rates, increased access to healthcare and pharmaceutical care, and improved health outcomes. Moreover, hospitals in expansion states have seen increased Medicaid revenue, decreased costs of uncompensated care, and states themselves have experienced reductions in disease-related deaths, and gains in life expectancy. Importantly, overwhelming evidence shows expansion has no negative effects on workplace engagement, and rather may help increase workplace success.
If the ability to work remains a prerequisite for care, I will spend my career watching patients suffer—not because I lack the skills to help them, but because the system forbids it. Practicing medicine under those rules doesn’t just make my job harder; it risks our patients losing faith in the system altogether.
The evidence is clear, we should be expanding Medicaid, not restricting it, for the good of our patients, our hospitals, and our country.
Hridaya Shah is a medical student based in Georgia passionate about expanding access to health insurance and addressing health disparities in her community.
Dr. Toby Terwilliger is an Atlanta-based hospitalist who serves as cochair of Georgians for a Universal Health Program and currently serves as a National Board Member of Physicians for a National Health Program.
Trump’s Pervasive Assault on America’s Health
The recent federal budget bill slashed $1.5 trillion from Medicaid and Medicare. Yet the Trump administration’s attack on health regulations and research extends much further, undoing decades of proven capacity to save lives and reduce disease. We must harness discontent with this assault on health to rebuild and improve the system.
The Dismantling of American Health Care, NY Review of Books, July 8, 2025, by Adam Gaffney, David U. Himmelstein, and Steffie Woolhandler
On July 4 President Donald Trump signed into law a piece of legislation that amounts to a declaration of war on the working-class and the sick. The “One Big Beautiful Bill Act” will slice more than $1 trillion from Medicaid over the next decade, stripping health coverage from more than 11 million lower-income Americans by 2034 and sending tens of thousands to an early grave—all in exchange for tax reductions for corporations and the wealthy. Despite Trump’s promises to the contrary, the law will also cut nearly $500 billion from Medicare over the same period by making the deficit surge past a point at which the Office of Management and Budget “is required to order a sequestration to eliminate the overage.”
This assault on the nation’s major public insurance programs is only the latest front in an ongoing right-wing campaign against health. On April 1 Trump’s hammer fell on the Department of Health and Human Services (HHS), the sprawling agency that encompasses the Centers for Disease Control and Prevention (CDC), the Centers for Medicaid and Medicaid Services (CMS), the National Institutes of Health (NIH), and the Food and Drug Administration (FDA), among other health-focused agencies. Having already forced out 10,000 HHS personnel earlier in his term, the Trump administration terminated 10,000 more on dubious legal grounds, devastating entire teams focused on major public health problems like tobacco control and occupational health. Altogether 25 percent of HHS’s workforce was dismissed. Since then a minority of the fired employees have been reinstated in the face of political pressure—but the depth and capriciousness of these chaotic cuts is without precedent. Disease surveillance, outbreak investigation, vaccine uptake, violence prevention, infection control, food safety, and opioid overdose prevention will likely suffer.
Meanwhile the nation’s biomedical research enterprise—in large part conducted by publicly financed scientists employed at universities— has been facing a sustained attack. NIH research grants that address important but now illicit health issues—like HIV/AIDS, racial health inequities, vaccine hesitancy, and LGBTQ health—have been wiped out in recent months. Not all of the cuts stem from specific bêtes noires: the administration has broadly decimated funding by canceling more than $1.8 billion in existing NIH grants in less than a month and a half (although some have been temporarily reinstated by court orders), reducing the issuance of new grant awards by 28 percent, and attempting to slash the “overhead” payments that cover universities’ costs for space and utilities via a now-stayed order that would have reduced grants from multiple federal agencies, including the NIH. This is on top of the funding blockades that the administration has imposed on many elite universities to bring them to heel—including all of the Ivies except Dartmouth and Yale.
The three fronts of this assault—on tax-funded medical coverage, public health, and medical research—have overlapping aims. The campaign to slash Medicaid—relied on by the poor since its establishment in 1965—follows a long neoliberal tradition of prescribing austerity for the working class and largesse for the rich. Trump and his allies seem to view public health, for its part, as waste that can be excised (DOGE-style) to fund tax cuts, as a source of regulatory excess that constrains profit-making, and as a locus of “woke” ideology and inconvenient facts. The assault on medical research is driven by similar concerns, with the added benefit of dominating rival centers of power like universities and the professions.
Yet such economic and ideological motivations do not explain the full measure of the administration’s agenda. It rests, too, on a Dark Ages disdain for science, part and parcel of Trump’s claim to be the arbiter of facts and truth. …
It seems difficult at present to resist Trump’s regressive anti-health juggernaut, much less to envision something better for tomorrow. But the medical community, which still wields considerable power and influence, appears to be reaching a boiling point. Colleagues fear seeing their coworkers and patients deported; academic freedom is threatened; medical decision-making is constrained by political fiat and managed care restrictions; research funding has disappeared; public health protections have been eviscerated; access to vaccinations has been curtailed; and charlatanism is displacing science at the highest level. Health professionals, having watched Congress slash the public insurance programs on which their patients and institutions rely, are soon to witness the needless suffering and death that will predictably follow. All these assaults are also breeding disaffection among voters. As many polls indicate, health is perhaps Trump’s weakest suit with the general public; most Americans favor more funding for science and public health, as well as universal coverage.
Comment:
By Jim Kahn, M.D., M.P.H.
This article is a tour-de-force review of the myriad ways that the Trump administration is undermining health care (especially public insurance), public health, and medical research. These are all areas that have yielded benefits to health over three-quarters of a century. The funding cuts have been massive, rapid, sometimes targeted, and often seemingly arbitrary. The cuts and their justifications often conflict or fail to withstand scrutiny. Further cuts are looming. As the article says, the actions bespeak a “Dark Ages disdain for science.”
For those interested in a survey of the anticipated effects of the budget bill on public insurance, in the context of health insurance trends, read Adam’s testimony to a Congressional committee.
At the end, Gaffney et al note that both the medical profession and voters dislike the broad assault on health care and science. We must hope that that this discontent will grow, and as political power shifts, we will soon have historic opportunities to rebuild, doubling down on our commitments to the public’s health, even – or especially – when that goal collides with the imperatives of maximizing shareholder value.
https://healthjusticemonitor.org…
Stay informed! Subscribe to the McCanne Health Justice Monitor to receive regular policy updates via email, and be sure to follow them on Twitter @HealthJustMon.
Medicare for All Explained Podcast: Episode 126
Medicare Stealth Cuts
Aug. 15, 2025
Additional episodes will be uploaded monthly. Subscribe in iTunes, or access a complete archive of the podcast, below.
Corporate Profit Trajectory Undermined US Health Care
In the latest installment of NEJM’s series on the Corporatization of US Health Care, a historian reviews the trajectory launched half a century ago that led to big business profits permeating our health system, to the great detriment of patients.
A Gilded Age for Patients? The Broken Promises of Profit-Driven Medicine, From the Series: The Corporatization of U.S. Health Care, The New England Journal of Medicine, August 2, 2025, by Nancy Tomes
Between the 1920s and the 1960s, the American medical profession developed a new doctor-controlled business model of care delivery, dependent on continual investment in new drugs, technologies, and procedures. That model created the profit opportunities that enticed corporate stakeholders to invest in health care in the 1970s and 1980s. But as the corporate presence increased, physicians lost control of their business model.
Hospitals had to function in a more efficient, businesslike fashion. That ethos spread to private practice as well. This financialization led to dynamics whose negative consequences persist to this day. Even the middle-class patients, who were expected to benefit most from medicine’s new model, found the costs hard to budget for and the world of medical specialization difficult to navigate. These discontents created the opening for new business partners: insurance companies, which in the late 1930s figured out how to profitably pool savings for unpredictable expenses.
The “merger movement” in hospital and physician services enabled health care organizations to benefit from economies of scale while minimizing direct price competition. Hospitals and physician practices slowly fused into chains.
Although it may seem obvious that health care doesn’t work like a restaurant chain, many powerful health care industry stakeholders still believe allowing corporate interests freer rein will produce that “golden age for patients.” The health care economy’s fragility suggests otherwise.
No market solution has arisen for the most critical determinant of poor health and health care outcomes in the United States: extreme income inequality. The Trump administration appears intent on blowing up our fragile health care system in the name of an unrestrained “free market” and corporate profiteering. Many people will suffer if the system collapses completely, but perhaps a more sustainable health care system can be built from the rubble.
Comment:
By Don McCanne, M.D.
With Trump’s affinity for gold Rococo, it seems like he may believe that this is “the golden age,” but not for patients, just for the billionaires. For patients, he would perpetuate “the most critical determinant of poor health and health care outcomes: extreme income inequality.”
There is no need to further elaborate on why we have the most expensive but poorest performing health care system. Historian Nancy Tomes provides a succinct summary. But based on decades of inertia in producing the reforms that would reverse the high cost/poor performance ratio, there is a clear need to reinforce the public’s understanding that there is a well-documented model of reform that would provide high quality care for absolutely everyone at a cost that each of us could afford. Need we say it? Of course that is a single payer national health program, sometimes referred to as an improved Medicare for All.
Isn’t it about time that we got with the program?
https://healthjusticemonitor.org…
Stay informed! Subscribe to the McCanne Health Justice Monitor to receive regular policy updates via email, and be sure to follow them on Twitter @HealthJustMon.
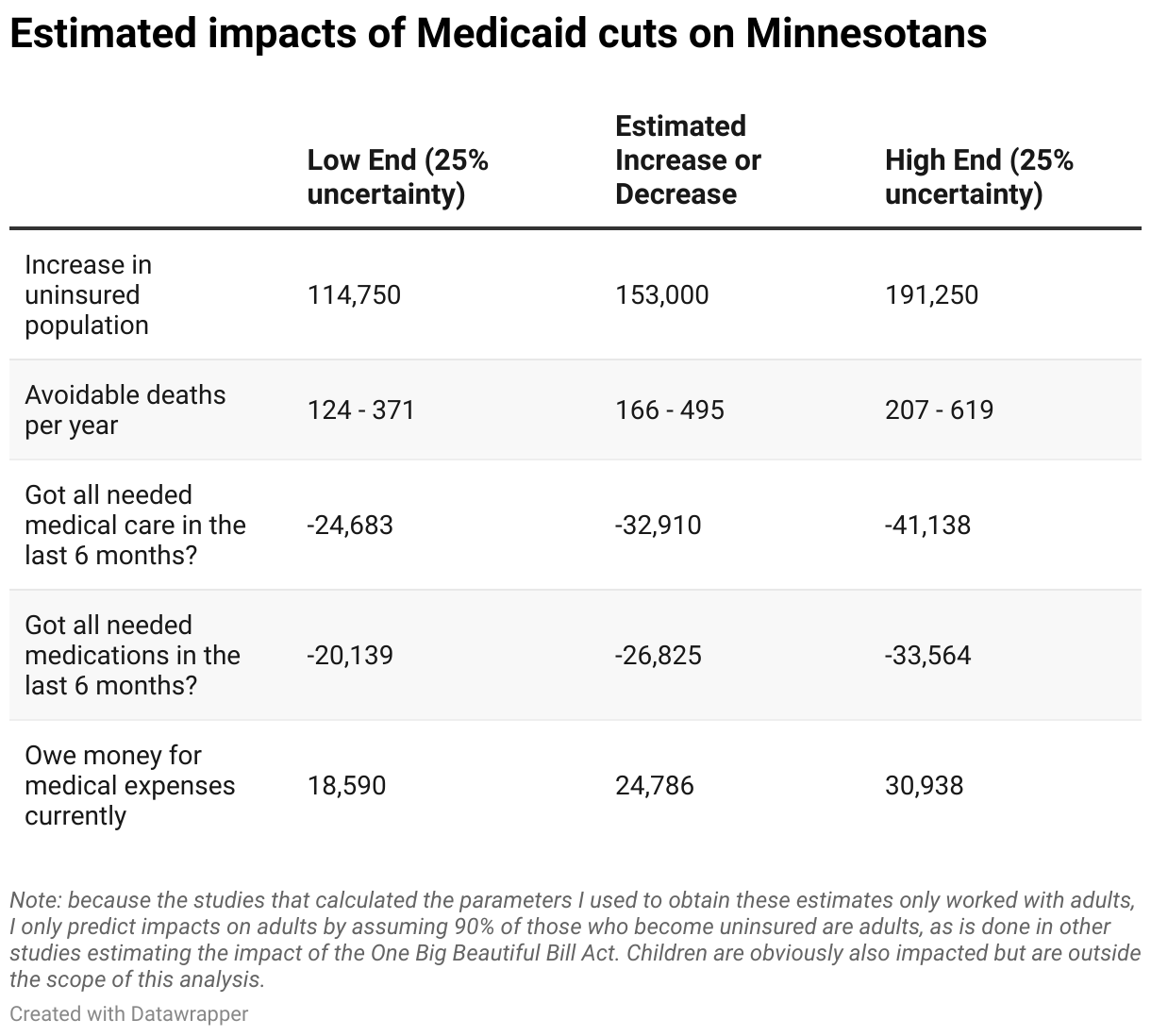
Here’s how many Minnesotans may die because of Congress’ Medicaid cuts
By Thomas Lane
Minnesota Reformer, Aug. 11, 2025
When we hear about health policy changes in the news, usually the numbers we hear are related to insurance: How many people will become insured or uninsured as a result of the latest legislation? Analysts — and as a result, news reporters, too — tend to use these numbers because they’re relatively simple to predict and understand.
But at the end of the day, health insurance is just a little card legally linked to a thick stack of paperwork in some office somewhere. Insurance numbers don’t really tell us much about what we actually want to know, which is the human health impact. How many medically avoidable deaths will a given piece of legislation prevent or cause? How many will or won’t get the care they need? How many more will or won’t be in medical debt?
Congress passed and on July 4 President Trump signed his “One Big Beautiful Bill Act,” the largest ever cut to government health care funding in U.S. history. The Congressional Budget Office projects the law will push about 10 million Americans off of health insurance while growing the deficit by $3.4 trillion over the next decade.
Health economists have studied the link between health insurance and health outcomes and can estimate how many more preventable deaths Americans will suffer as health coverage declines, among other outcomes.
The Minnesota Department of Human Services recently released preliminary estimates that about 140,000 Minnesotans will lose their health insurance as a result of the legislation.
Additionally, due to upcoming subsidy expirations and rule changes for the Affordable Care Act’s insurance markets (“Obamacare”), health policy analysts at KFF have predicted an additional 5.1 million Americans will become uninsured nationwide, leading to an additional 13,000 uninsured Minnesotans.
Using this 153,000 figure, we can estimate that roughly one more Minnesotan will unnecessarily die per day as a result of losing coverage. Tens of thousands more will forego necessary care, miss medications, and rack up medical expenses they cannot afford.
Make no mistake, however. The craziest part of all of this should not be these figures themselves. It’s the fact that they can mostly still be prevented from coming to fruition by our state Legislature.
KFF estimates that the One Big Beautiful Bill Act is expected to cost the state up to $2.4 billion per year over the next decade, leaving a big hole for our state legislators to fill. Although some of these harms are caused by Congress’s imposition of work requirement paperwork burdens on Medicaid beneficiaries that the state cannot do much about, most of them come from the funding cuts, and funding cuts are something the state can definitely do something about. Minnesota just needs to come up with roughly $2.4 billion on its own.
How exactly can the state find such a large sum of money — roughly 6% of the state general fund budget? Believe it or not, it’s not actually that complicated. Currently, the state runs Medicaid through private third-party administrators called managed care organizations, or MCOs. These MCOs are a product of the 1990s, when the public policy world thought the problem with health care was that people were using too much of it, and health care needed gatekeepers.
It’s a rather evidence-free claim. Consider that Americans actually use less care than people in Europe and Canada despite spending far more per capita than them, all while also living shorter, less healthy lives. Nonetheless, the MCOs still run Minnesota’s Medicaid program, adding significant administrative expenses onto the state budget while doing nothing to make health care better.
Connecticut got rid of these wasteful MCO contractors in 2012, instead opting to run its Medicaid program itself. Unsurprisingly, they saved lots of money doing so. How much would Minnesota save if it spent per beneficiary what Connecticut does on Medicaid? About $1.5 billion annually, according to my analysis.
Given the $2.4 billion in cuts also includes some money cut from non-health care areas, that $1.5 billion in savings is likely enough to fill most of the health care-related hole in the state budget! With that money, the state can ensure tens of thousands of Minnesotans get the care they need while preventing closures of Minnesota hospitals and nursing homes that depend on Medicaid for funding.
During the last legislative session, I wrote a column in support of legislation called the Patient-Centered Care bill that would more or less copy what Connecticut did (SF1059/HF255). Unfortunately, neither the state House nor Senate brought it up for serious consideration.
Back then, it was admittedly still uncertain whether Congress would actually pass massive cuts to Medicaid, but it did, and now there are no more excuses. Our state Legislature can quite easily alleviate most of the financial problems Congress has passed onto it and thereby save lives.
All they have to do is pass a not very big but in my opinion quite beautiful bill to cut wasteful MCO middlemen out of our Medicaid program.
Budget Bill Sabotages Medicare
Senator Sheldon Whitehouse provides a perfect, concise explanation of the Congressional sneak attack on Medicare: The budget bill added $3.5 trillion to US debt, mainly to fund tax cuts for billionaires. This automatically triggers $535 billion in cuts to Medicare.
$535 billion in cuts to Medicare. Republicans fingerprints are all over it, U.S. Sen. Sheldon Whitehouse (Rhode Island), YouTube short (90 seconds)
Comment:
By Jim Kahn, M.D., M.P.H.
Sen. Whitehouse regularly and powerfully calls out Republican complicity and hypocrisy. In this brief clip from a Senate floor speech, he reveals how the recent budget reconciliation bill – aside from slashing Medicaid by $1 trillion via explicit cuts – also generates massive Medicare cuts. As he explains, huge tax cuts for the rich bump up the federal budget deficit by trillions of dollars, leading to an automatic “sequestration” of funds for Medicare. We’ve mentioned this in HJM, but Sen. Whitehouse’s adept rhetorical style really drives home the point.
Circulate it widely. It exposes how Republicans are dismantling health care for the elderly and disabled, not just for the poor.
https://healthjusticemonitor.org…
Stay informed! Subscribe to the McCanne Health Justice Monitor to receive regular policy updates via email, and be sure to follow them on Twitter @HealthJustMon.
Consensus Statement on Expanding Prior Authorization in Traditional Medicare
Aug. 5, 2025
We, the undersigned organizations and individuals, issue the following consensus statement regarding the Wasteful and Inappropriate Services Reduction (WISeR) model recently proposed by the Center for Medicare and Medicaid Innovation to begin January 1, 2026.
Background
The WISeR model proposes to implement prior authorization for at least 17 additional services in traditional Medicare (TM) in six states. The model will solicit applications from private companies that currently administer prior authorizations for private health insurers, including Medicare Advantage (MA) plans. The model will run for 6 years.
Shared Perspective
As former government officials, providers, policy experts, researchers, and patients, we are concerned about the design of the model and recommend it not be initiated. Our specific concerns are outlined below.
1. Participant payment model: The WISeR model proposes to compensate the private companies participating “based on a share of averted expenditures.” This payment structure immediately creates an incentive for companies to avert more expenditures by denying more prior authorization requests in order to increase their compensation. Evidence from government agencies and experts across the political spectrum has demonstrated that MA prior authorization, which also results in additional retained revenue when care is denied, very often improperly denies care. (1,2) A participant payment model that mirrors the current incentives in MA is likely to fall victim to the same misaligned incentives and lead to delays and denials of needed care.
2. Participant selection: The model intends to allow participants who are currently administering prior authorization processes for private payers, including MA companies. Currently, the Medicare Administrative Contractors (MACs) that administer prior authorizations in TM have an accuracy rate of over 98%. (3) Further, MAC prior authorization decisions are overturned less than half as frequently (roughly 35%) as decisions made by private companies administering MA prior authorization with an 81.7% overturn rate. (4) Thus, the participants desired for the WISeR model have demonstrated inferior performance in making accurate prior authorization decisions, which have resulted in serious harm and death to patients. (5) These same bad actors should not be given the ability to make these decisions in TM.
3. Prior authorization protocols: The lack of transparency in MA prior authorization makes it impossible to justify expanding these processes into TM, based on evidence of their accuracy or benefit to patients and providers. MA insurers do not report prior authorization decisions based on type of service, contract, or reason for denial. Additionally, the protocols used to review prior authorizations in MA are not disclosed to patients, providers, or policymakers. Given that prior authorization in MA is a black box with documented adverse effects on patients and moral injury to providers, expanding the process without a full public audit of how it is currently conducted with recommendations for improvement is risky. (6)
4. Use of enhanced technology: The model references the use of enhanced technologies for prior authorization review. However, these technologies, particularly the use of artificial intelligence (AI) systems, have been associated with significantly higher rates of care denials. For instance, internal documents from MA insurers demonstrate that denials for post-acute care services rose sharply following the implementation of AI-driven review processes administered by naviHealth, a subsidiary of UnitedHealth Group. (7) Often these denials in MA are inappropriate as the Department of Health and Human Services Office of the Inspector General and whistleblowers have demonstrated. (8,9) This, combined with the lack of transparency into the methodologies behind the enhanced technologies used by private insurers (the intended model participants) could result in delays and denials of needed care for seniors and people with disabilities enrolled in TM.
Signed,
Center for Health and Democracy
Physicians for a National Health Program
Public Citizen
Center for Medicare Advocacy
Robert Berenson, MD, Former Commissioner of the Medicare Payment Advisory Commission
Donald Berwick, MD, Former Administrator, CMS
Andrea Ducas, MPH, Vice President for Health Policy, Center for American Progress
Clifton Gaus, ScD, Former Administrator of Agency for Health Care Policy and Research (now AHQR)
Richard Gilfillan, MD, Former Director, Center for Medicare and Medicaid Innovation
Ed Weisbart, MD, National Board Secretary, Physicians for a National Health Program
Bruce C. Vladeck, Administrator, Health Care Financing Administration, 1993-1997, Board Chair Emeritus, Medicare Rights Center
Judy Feder, Professor and former Dean, McCourt School of Public Policy, Georgetown University
This statement was sent to the U.S. Department of Health and Human Services, the Centers for Medicare and Medicaid Services, and the Congressional staff members on Aug. 5, 2025.
References
- U.S. Department of Health and Human Services, Office of Inspector General, Some Medicare Advantage Organization Denials of Prior Authorization Requests Raise Concerns About Beneficiary Access to Medically Necessary Care, report no. OEI-09-18-00260, April 2022, https://oig.hhs.gov/reports/all/2022/some-medicare-advantage-organization-denials-of-prior-authorization-requests-raise-concerns-about-beneficiary-access-to-medically-necessary-care/.
- Jeannie Fuglesten Biniek, Nolan Sroczynski, Meredith Freed, and Tricia Neuman, “Medicare Advantage Insurers Made Nearly 50 Million Prior Authorization Determinations in 2023,” KFF (January 28, 2025), https://www.kff.org/medicare/issue-brief/nearly-50-million-prior-authorization-requests-were-sent-to-medicare-advantage-insurers-in-2023/.
- U.S. Centers for Medicare & Medicaid Services, Prior Authorization and Pre‑Claim Review Program Statistics for Fiscal Year 2023, January 17, 2025, https://www.cms.gov/files/document/pre-claim-review-program-statistics-document-fy-23.pdf
- Jeannie Fuglesten Biniek, Nolan Sroczynski, Meredith Freed, and Tricia Neuman, “Medicare Advantage Insurers Made Nearly 50 Million Prior Authorization Determinations in 2023,” KFF (January 28, 2025), https://www.kff.org/medicare/issue-brief/nearly-50-million-prior-authorization-requests-were-sent-to-medicare-advantage-insurers-in-2023/.
- Jennifer Lubell, When Prior Authorization Blocks Lifesaving Treatments, American Medical Association (April 7, 2025), https://www.ama-assn.org/practice-management/prior-authorization/when-prior-authorization-blocks-lifesaving-treatments.
- U.S. American Medical Association, 2024 AMA Prior Authorization (PA) Physician Survey (American Medical Association, 2024), https://www.ama-assn.org/system/files/prior-authorization-survey.pdf
- U.S. Senate Permanent Subcommittee on Investigations, Refusal of Recovery: How Medicare Advantage Insurers Have Denied Patients Access to Post‑Acute Care, Majority Staff Report (October 17, 2024), https://www.hsgac.senate.gov/wp-content/uploads/2024.10.17-PSI-Majority-Staff-Report-on-Medicare-Advantage.pdf
- U.S. Department of Health and Human Services, Office of Inspector General, Some Medicare Advantage Organization Denials of Prior Authorization Requests Raise Concerns About Beneficiary Access to Medically Necessary Care, OEI‑09‑18‑00260 (April 2022), https://oig.hhs.gov/reports/all/2022/some-medicare-advantage-organization-denials-of-prior-authorization-requests-raise-concerns-about-beneficiary-access-to-medically-necessary-care/.
- Casey Ross and Bob Herman, “UnitedHealth Pushed Employees to Follow an Algorithm to Cut Off Medicare Patients’ Rehab Care,” STAT (November 14, 2023), https://www.statnews.com/2023/11/14/unitedhealth-algorithm-medicare-advantage-investigation/.
Medicare and Medicaid at 60
The contribution of Medicare and Medicaid to American life cannot be overstated. Almost one in four Americans is on Medicaid, including over 40% of children.
By Walter Tsou, M.D., M.P.H.
The Philadelphia Inquirer, July 30, 2025
Sixty years ago today, President Lyndon Johnson signed into law the two most consequential health programs in U.S. history — Medicare and Medicaid. Both Medicare (Title 18) and Medicaid (Title 19) were added to the Social Security Act with benefits directed at seniors.
For seniors no longer in the workforce and those who were chronically disabled, Medicare, along with Social Security, were the programs that allowed the elderly not to fall into abject poverty at a time when their health worsened.
Medicaid was created from the federal-state partnership of the 1960 Kerr Mills Act, but Congress expanded the age limits of eligible low-income populations to include families with children, people with disabilities, and the blind.
Wilbur Cohen, undersecretary of the Department of Health, Education and Welfare under Johnson, is considered the father of these two essential programs. Cohen envisioned a national health insurance program for America, but, given the power of the medical and insurance lobby, had to settle for Medicare for seniors and Medicaid for low-income citizens. He likened the final legislation to the salami approach, where he would accept one slice at a time until he could get the whole salami.
Sixty years later, we are still waiting.
The contribution of Medicare and Medicaid to American life cannot be overstated. Today, all seniors with 40 quarters of Medicare taxes paid, those with chronic disabilities, ALS, and patients on dialysis, are covered by Medicare. We only need to imagine if coverage had not been expanded, what a difference it would make to family finances, work productivity, or premature mortality.
Almost one in four Americans is on Medicaid, including over 40% of children. The proposed work requirements and new paperwork verifications needed to retain Medicaid —thanks to the recently enacted “big, beautiful bill” — will make our current bureaucratic and dysfunctional approach to healthcare financing even worse — actually far worse.
In Arkansas, a work requirement cost the state $26 million without any increase in employment or volunteer time. Even worse, more than 18,000 lost health insurance coverage. Now multiply the new unfunded mandate on each state government that must verify this new onerous paperwork requirement, and add the millions who are predicted to lose their health insurance, and you realize that we are moving dramatically away from the original intent of Medicare or Medicaid.
Despite the belief that markets are more efficient, in healthcare, it makes it much more cumbersome and dysfunctional.
In 1948, the Universal Declaration of Human Rights was adopted by the U.N., including the United States. Article 25 states that “everyone has the right to a standard of living adequate for the health and well-being of himself and of his family.” Two points should be emphasized. Everyone means that if you can breathe, regardless of your position in life, a society has a basic level of care that is provided to you. Second, universal health insurance or access to care is essential for health.
Beyond the recognition that healthcare is a human right, it is a necessity for a productive society. Our taxes are dependent on people well enough to work, play, and worship. Keeping people insured keeps them well. Keeping them well keeps our society productive.
We have unfortunately believed that market forces can solve all that is wrong in healthcare. Some think we can solve our labor shortages by forcing the few “able-bodied” to be required to work or by denying emergency care to immigrants.
Meanwhile, we ignore the real “waste, fraud and abuse” in the system by the tens of billions overcharged by Medicare Advantage plans or the private equity schemes that bankrupted Crozer Chester and Taylor hospitals or Hahnemann.
The “big, beautiful bill” was supposed to cover only the original intent of the Medicare and Medicaid program. Instead, it will destroy the fragile infrastructure of healthcare.
Maybe we need a new guiding principle on this anniversary: Healthcare is a public good, not a market commodity, and we should finally get that big salami.
Dr. Walter Tsou is a former health commissioner of Philadelphia and a national board adviser to Physicians for a National Health Program.
Looming ACA Premium Hikes … A Political Hot Potato
Enhanced tax credits for ACA exchange plans will expire this year, leaving 20 million people facing premium hikes of 75% ($1000). The GOP, which delayed their Medicaid cuts to try to avoid voter backlash, has a new problem not of their making. What will they do?
Individual market insurers requesting largest premium increases in more than 5 years, Peterson-KFF Health System Tracker, July 18, 2025, by Jared Ortaliza, et al.
… The costs of health care services like hospitalizations and physician care, as well as prescription drug costs tend to go up every year, and insurers often raise premiums to cover their increased costs. For 2026, insurers commonly say the underlying cost of health care (medical trend) is similar to last year’s reported 8%. …
Another change expected for next year is the enhanced [ACA] tax credits are set to expire. … For the last five years, enhanced premium tax credits have increased the amount of financial assistance enrollees in ACA Marketplace coverage receive, lowering their monthly premium payments. If Congress takes no action to renew these enhanced tax credits, enhanced subsidies will expire at the end of 2025, which will cause premium payments for subsidized enrollees to increase by over 75% starting in January 2026. Insurers expect a large share of enrollees to leave the market, and that those enrollees will be healthier on average, thus leaving the risk pool sicker on average.
Inflation Reduction Act Health Insurance Subsidies: What is Their Impact and What Would Happen if They Expire?, KFF, July 26, 2024, by Jared Ortaliza, et al.

Memo advises GOP to extend ACA tax credits, The Hill, July 22, 2025, by Alejandra O’Connell-Domenech, et al.
A new memo from Plymouth Union Public Research … advises Republicans that the best way to fend off attacks from the left about Medicaid cuts is to extend ObamaCare’s enhanced premium tax credits. …
The memo notes that all benefits [to taxpayers] from tax cuts will be nullified because of premium increases if the subsidies are not extended.
PUP Research is the sister group to PUP Advocacy, a conservative advocacy organization.
Extra subsidies that help people afford ObamaCare premiums that were put in place during the coronavirus pandemic are set to expire at the end of the year, and there are few signs Republicans are interested in tackling the issue at all.
If Congress takes no action, premiums for subsidized enrollees are projected to increase by more than 75 percent starting in January 2026, according to health research group KFF.
There is broad bipartisan and public support for extending the subsidies, and the memo cited recent polling from Trump pollster Fabrizio Ward that showed Republicans losing support in the most competitive districts if the tax credits expire.
But if Republicans extend them, the poll showed they can gain an advantage against Democrats in the midterms. The Republican candidate that supports extending the tax credits would lead the Democrat on the generic ballot by 6 points overall.
Comment:
By Jim Kahn, M.D., M.P.H.
The recently passed federal budget bill imposes massive cuts to Medicaid and Medicare, close to $1.5 trillion. The Medicaid cuts, mainly in eligibility criteria, start only after the Congressional mid-terms, shielding Republicans from voter backlash. The Medicare cuts arise from budget shortfalls caused by the massive tax cuts (tilted to the rich, of course).
Also happening through inaction is the expiration of COVID-era strengthening of ACA exchange plan subsidies (premium tax credits). As shown in the figure below, ACA enrollment rose sharply from 2020 to 2024, reaching 20 million subsidized individuals. The credits are set to expire in 2025. This will leave tens of millions of people in the lurch: experiencing a massive increase in costs – 75% higher premiums, about $1000, according to KFF analyses above. This will happen before the 2026 midterms, and be blamed on the GOP, likely exacting a significant toll at the ballot box
Republican strategists have noticed – as reported by The Hill, above. So of course they are encouraging a (short) extension of the subsidies. Which would place the Democrats in a political pickle – support the right policy, even if may hurt you in the next election.
No political party wants the hot potato of cutting insurance benefits, so they try to avoid credit (actually, blame). Wouldn’t it be spectacular if we were all covered, with the same cradle-to-grave universal health plan? Generous and efficient. Fairly funded. Single payer.
https://healthjusticemonitor.org…

Stay informed! Subscribe to the McCanne Health Justice Monitor to receive regular policy updates via email, and be sure to follow them on Twitter @HealthJustMon.
Medical funding should be a social good
By Henry Kahn, M.D.
The Atlanta Journal-Constitution, Letters, July 28, 2025
As explained by Mike King in his AJC Opinion piece, “Why a beloved hospital failed – and why it doesn’t have to be this way,” July 20, the Atlanta Medical Center came to its end because it couldn’t survive in our country’s environment of profit-oriented medical care.
King is correct. The United States stands out among all wealthy societies as the only place where health and medical care are supposed to exist as businesses. In other wealthy countries, it’s presumed that health is – and should be – a social good, not a commercial product.
Those societies pay for their doctors, nurses, clinics, hospitals and public health services through progressive taxation plans that save money for the population. They don’t permit high overheads, lobbying or skimming profits off every collected dollar. Their medical coverage is essentially universal (everybody included in the same plan) because that’s the ethical and less expensive solution.
Medical funding in Georgia and the U.S. Is in a gloomy place right now. A bright spot can be found among the younger doctors, nurses and trainees who won’t accept the commercial distortion of their duty to deliver care where it’s needed. It’s time for our politicians and bean counters to follow the lead of the more Idealistic, coming leadership.