Summary: As the US approaches 800,000 COVID deaths, this week we review how pandemic control fared in two countries. Today: Taiwan, where broad public cooperation coupled with technical finesse to minimize health and economic harm. On Wednesday: the US, where pandemic response was hobbled by tense interactions between political partisanship and public health.
How has Taiwan navigated the pandemic?, Economics Observatory, December 1, 2021, by Tsung-Mei Cheng
Taiwan has fared better than many other countries during the Covid-19 crisis. Political leadership, early action, a national plan, strong information and communications technology infrastructure and a cooperative public have all contributed.
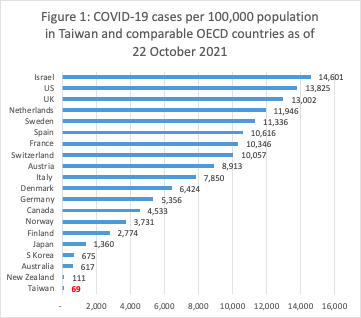
As of October 2021, Taiwan ranked lowest in total number of Covid-19 cases and second lowest in deaths per 100,000 population among comparable OECD countries.
Of 20 nations, the United States ranked second with 13,825 cases per 100,000 population and Taiwan ranked twentieth with 69 per 100,000. … the United States ranked first with 224 deaths per 100,000 population and Taiwan ranked nineteenth with 4 per 100,000.
{kind=link}
At the same time, Taiwan’s economy grew in both 2020 and 2021. This continued, and even outpaced, the growth seen in preceding years. In contrast, the world’s real GDP declined by 3.4% in 2020, with the G20 countries, members of the euro area and comparable OECD countries had negative growth ranging from -1% to -11%.
The situation has remained stable since the government lowered the emergency alert from level 3 to level 2 on 27 July 2021. Since September, new cases of domestic transmission have been at either zero or in the low single digits. Deaths have also remained very low. For nine successive days between 29 September and 8 October, Taiwan reported no deaths. This was at a time when the average daily deaths in the United States stood at 1,867, with most days exceeding 2,000 deaths per day.
Taiwan was prepared and acted at the first signs of the virus in early 2020. Policy makers had learned lessons from the 2003 SARS crisis and made plans to prepare for future pandemics.
To that end, the government strengthened Taiwan’s CDC and healthcare delivery system, and taught the public the importance of face masks, hand hygiene and temperature checks. In addition, a 2011 constitutional ruling granted the government power to do all that is necessary in national public health emergencies, including ‘temporarily removing personal freedom of movement’. This made mandatory quarantine possible during the Covid-19 crisis.
Difficulties frequently encountered in many Western countries with vaccine hesitancy, contact tracing, quarantine and facemask resistance have not generally been problems in Taiwan. The public regards cooperating with the government in national emergencies as a civic responsibility and shares the recognition that everyone is in this together. The importance of these two attributes cannot be overstated in Taiwan’s highly successful Covid-19 outcomes to date.
Comment:
By Don McCanne, M.D. (with all due credit to Tsung-Mei Cheng and Uwe Reinhardt)
There has been considerable disagreement within the United States about the nature of the Covid-19 epidemic, a disagreement not shared in Taiwan where the people worked together to try to bring it under control.
It is interesting that the author, Tsung-Mei Cheng, and her late husband, Uwe Reinhardt, worked with Taiwan to help establish their single payer health care financing system — a system that proved to be very helpful during this epidemic, along with their other public policies. Their ethical principles helped make the Taiwanese government much more effective in combating the scourge of Covid-19 than we were in the United States, in spite of our wealth.
In a Princeton Policy Podcast, Tsung-Mei Cheng said, “Uwe writes in the book (‘Priced Out’), and I’ll paraphrase him, health reform as in Europe, Canada, or say Taiwan, which operates a government-run single payer health care system; they usually begin their debate on health reform making explicit the ethical principles that should govern or constrain their health policy. They explicitly state what these ethical values are. For example, in Germany, the word is solidarity. Everybody respects that, and there is agreement on that. Say… yes, we want solidarity therefore everyone shall have health care, the same health care. Well, Canada, in the Canada Health Act, it says that all shall have health care based on health care needs and not on ability to pay. Now, in this country, Uwe’s experience has been that, you know, by merely bringing up the topic of distributive ethics for health care it can easily raise the ire of an audience because it is viewed as too personal, too political, or too divisive. So, instead, we discuss health reform mainly in technical terms, usually in economic terms and let social ethics fall where they may, and people certainly have different social ethics. Now the second biggest takeaway from the book for me is about what Uwe said about the uninsured in America. He said, and this is a direct quote from him, ‘The issue of universal coverage is not a matter of economics; little more than one percent of GDP assigned to health care could cover all. It is a matter of soul.’”
Well, this is embarrassing. We, as a people, have it within our power to address these problems effectively – not just Covid, but health care for the entire nation, forever. What do we do? Well, for Covid, we’ll soon be approaching a million deaths. And all of our other health problems? For shame, America. For shame!
http://healthjusticemonitor.org…
Stay informed! Subscribe to the McCanne Health Justice Monitor to receive regular policy updates via email, and be sure to follow them on Twitter @HealthJustMon.