By Stephen Kemble
OpEd News, November 16, 2011
Many still assume universal health care must mean higher costs, but other countries prove this assumption false. The US spends about twice as much per capita on health care as other industrialized countries, yet others are able to cover everyone and have better health outcomes. If we are to succeed in health care reform, we must ask the question, “What are we spending on health care that other countries are not, and that does not add value to health care?” We are now spending about 18% of our gross domestic product on health care and rising. If we do not correctly identify wasted spending and take steps to reduce it, health care spending will continue to break the budget. Contrary to what some assume, all evidence indicates that government financing in health care is actually far more efficient than the private insurance industry. The “Patient Protection and Affordable Care Act” (PPACA) is built around the private insurance model with government subsidies to fill in some of the gaps. It will not reduce total national health spending or waste, and we will face escalating pressure to restrict necessary care.1,2
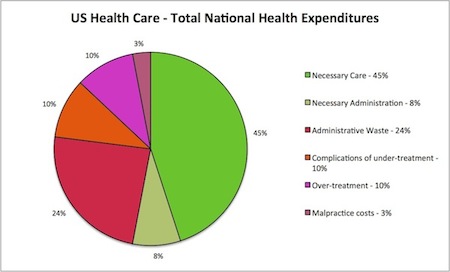
This Pie Chart is based on evidence from comparison with other countries that have well functioning national health plans, 3,4 from cost analyses of various national and state level health reform proposals, including the PPACA, done by The Lewin Group,2 the Congressional Budget Office (CBO), and Centers for Medicare and Medicaid Services (CMS),1 and from studies on regional variations in health care spending in the US. 5 The percentages are estimates, but based on available evidence they are “in the ballpark.” The data is much firmer for administrative costs than for unnecessary and inappropriate care.
Administrative Waste (est. 24%)
Administrative waste is the difference between what the U.S. spends on health care administration and what countries with efficient universal systems spend.3,4 Administrative costs include health insurance administration (premiums collected minus payments to health care providers), and administrative costs for doctors, hospitals, employers, and the public.
The “waste” includes marketing and advertising, underwriting, multiple private bureaucracies, highly paid executives, managed care costs, pharmacy benefit manager costs, maintenance of insurance reserves, profit, lobbying and “government relations,” employer and broker costs, costs to doctors and hospitals to deal with billing and insurance, and physician time lost to dealing with prior authorizations and formulary restrictions.
All of these are directly attributable to use of competing private insurance plans, and especially for-profit insurance companies, to finance health care. None add any measurable value to health care.
Unnecessary and Inappropriate Care (est. 20%)
Unnecessary and inappropriate care is due to inadequate access to necessary care (under-treatment), or to various forms of over-treatment. There is actually far more under-treatment than over-treatment in the U.S.,6 but much of it is in the form of unnecessary suffering and death due to lack of access to care that does not show up in cost figures.
Under-treatment results from lack of insurance, under-insurance, and inadequate access to primary care, leading to excessive use of emergency services and delay in disease treatment resulting in expensive complications and preventable hospitalizations. It also includes medical errors and inefficient care due to pressure on physicians to spend inadequate time with patients, leading to failure to listen and think through problems to provide the best care.
Over-treatment includes procedures and services driven by provider profit motive, rather than the best interest of the patient, and irrational reimbursement policies and misallocation of health care resources according to profit incentives rather than health care needs of the population. It includes direct to consumer advertising leading to inappropriate patient demand for care, especially for drugs. It includes defensive medicine due to fear of lawsuits. It also includes provider fraud.
All of these are much more difficult or impossible to address in a fragmented health care market. In health care, the evidence shows that competition among insurance companies and fragmentation of health care financing add administrative costs, drive up health care prices, impede access to necessary care, fail to reduce unnecessary care, impede detection of errors and fraud, and do not provide fiscal efficiency or add value to health care.7 The insurance exchanges in the PPACA may increase coverage, but add substantial administrative costs and cannot solve our cost problems.8,9
Other proposals to control costs, including health information technology, prevention, and comparative effectiveness research, may improve health care but are likely to cost as much as they save and will not “bend the curve” of escalating health care costs.10 Reorganization of doctors and hospitals into “accountable care organizations” and pay for performance schemes that shift insurance risk onto providers may reduce over-treatment, but bring an equally problematic and costly incentive for providers to under-treat and avoid taking on sicker and more complex patients. Reforms that target unnecessary care but rely on new layers of administration or use blunt strategies that restrict necessary as well as unnecessary care cannot make health care more cost-effective. Neither can reforms that push increasingly unaffordable costs onto those needing care, deterring more necessary than unnecessary care.
According to the CBO, malpractice costs are less than 3% of the US health care dollar. Tort reform proposals touted by the AMA are not likely to save more than 1% of health care costs at best.11
Only a universal publicly financed healthcare system could actually provide comprehensive coverage to all, free choice of doctors and hospitals, and reduced cost. Administrative waste could be eliminated off the top, and access to necessary care would improve substantially. The experience of other countries shows that a universal system would reduce or eliminate many of our perverse incentives for over-treatment, even if doctors are paid with fee-for-service. A system-wide quality improvement program with physician leadership could reduce unnecessary care more effectively than strategies now employed by insurance companies or proposed under the PPACA. Health care prices could be reduced in proportion to administrative savings without harming providers of care, and eliminating fiscal waste would greatly reduce pressure to limit benefits and deny and ration care. With a universal system, health care could be removed from injury litigation, markedly reducing both the size of judgments and the necessity to sue for access to injury related health care, eliminating more than half the cost of medical malpractice, worker’s compensation, and automobile insurance.
We are told that universal publicly financed health care is “off the table.” We need to get it back on.
Dr. Stephen Kemble is assistant professor of medicine at the University of Hawaii John A. Burns School of Medicine, and also in private practice as a general adult psychiatrist. He is a member of Physicians for a National Health Program. In September he was appointed by Hawaii’s Gov. Neil Abercrombie to the Hawaii Health Authority, charged with designing and then running a universal health care system for Hawaii.
References
1. Foster RS. Estimated Financial Effects of the “Patient Protection and Affordable Care Act,” as Amended. Centers for Medicare & Medicaid Services, O
ffice of the Actuary. April 22, 2010.
2. The Lewin Group. Patient Protection and Affordable Care Act (PPACA): Long Term Costs for Governments, Employers, Families and Providers. June 2010. http://www.lewin.com/publications/Publication/409/
3. Woolhandler S, Campbell T, Himmelstein D. Costs of Health Care Administration in the United States and Canada. N Engl J Med 2003;349:768-75.
4. Morra D, Nicholson S, Levinson W, Gans DN, Hammons T, Casalino LP. US Physician Practices vs. Canadians: Spending Nearly Four Times as Much Money Interacting With Payers. Health Affairs 30 , no. 8 (2011): doi: 10.1377/hlthaff.2010.0893
5. Fisher ES, Bynum JP, Skinner JS. Slowing the Growth of Health Care Costs — Lessons From Regional Variation. N Engl J Med. 2009 Feb 26;360(9):849-52.
6. Elizabeth A. McGlynn et al., The Quality of Health Care Delivered to Adults in the United States. N Engl J Med 2003;348:2635-2645, 2641.
7. Kuttner R. Market-Based Failure – A Second Opinion on U.S. Health Care Costs. N Eng J Med 2008;358:549-551.
8. Jost TS. Health Exchanges and the Affordable Care Act: Key Policy Issues. The Commonwealth Fund, July 2010.
9. Nardin R, Himmelstein D, Woolhandler S. Massachusetts’ Plan: A Failed Model for Health Care Reform. PNHP, Feb 18, 2009. https://pnhp.org/mass_report/mass_report_Final.pdf
10. The Obama Administration’s Options for Health Care Cost Control: Hope versus Reality. Ann Int Med 2009;150:485-489.
11. Mello MM, Chandra A, Gawande AA, Studdert DM. National Costs Of The Medical Liability System. Health Affairs 29, No. 9 (2010): 1569–1577.
http://www.opednews.com/articles/1/U-S-Health-Care-Spending-by-Stephen-Kemble-111116-331.html