From Dr. Don McCanne, MD
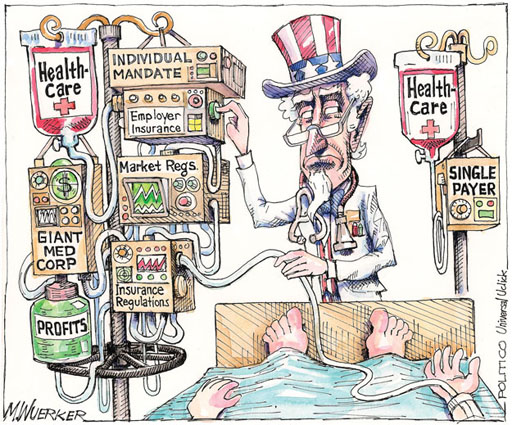
In a single cartoon, Politico’s Matt Wuerker demonstrates the U.S. health care system as it is, and as it should be.
Click on this Kaiser Health News link:
http://www.kaiserhealthnews.org/cartoons/2012/March/Drip.aspx
From Dr. Don McCanne, MD
In a single cartoon, Politico’s Matt Wuerker demonstrates the U.S. health care system as it is, and as it should be.
Click on this Kaiser Health News link:
http://www.kaiserhealthnews.org/cartoons/2012/March/Drip.aspx
In a single cartoon, Politico’s Matt Wuerker demonstrates the U.S. health care system as it is, and as it should be.
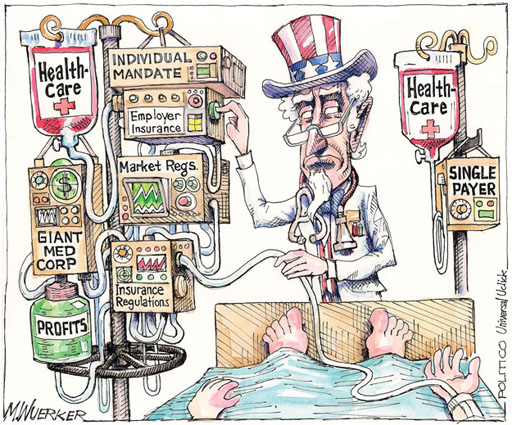
Click on this Kaiser Health News link:
http://www.kaiserhealthnews.org/cartoons/2012/March/Drip.aspx
By Marvin Malek, M.D.
Vermont for Single Payer, March 12, 2012
Vermonters are now being subjected to the most intense, well-funded propaganda campaign I have ever seen in Vermont.
Beginning in January of this year, the group, Vermonters for Health Care Freedom (VHCF), began to carpet bomb the airwaves with a media campaign targeting Act 48, the health reform law signed into law last May. The campaign uses the standard propaganda techniques of fear-mongering, distortion, and appeal to conspiracy theories.
Reality Check
The ads allege that a secret cabal of health reformers plan to raise our taxes by $5 billion to fund the new single payer system, that these conspirators already know how they plan to impose these taxes, and that they are hiding this information from the public.
Every element of this message is nonsense. Here’s the reality check:
$5 billion represents total health spending in Vermont currently. As is the case in most states, over half of Vermont’s health care money comes from federal sources. This includes funding for federal employees, the military, the VA, Medicare, and the majority of Medicaid funding. And Act 48, the reform bill, has been designed to ensure that we continue to receive all of the federal funding we normally receive. Furthermore, most of the remainder of the $5 billion is money we’re already raising. This encompasses out-of-pocket spending, health insurance premiums, and local and state taxes that are already funding health care for state and local employees, teachers, prisoners, VScript, Catamount, and Vermont’s portion of Medicaid spending.
So whatever additional revenue is required will represent only a small fraction of total health spending—not even close to $5 billion.
The ads never mention that Green Mountain Care—the proposed single payer plan– does not go into effect until 2017. Think about it: Is it realistic to expect those who are just beginning work on the reform effort to have already determined its entire funding structure—five years in advance? And that there is some sort of conspiracy related to Green Mountain Care’s funding for 2017? Next thing you know, they’ll claim a conspiracy if the Agency of Transportation or the Corrections Dept are unable to announce their 2017 budgets five years in advance.
Get real.
The truth is that the reform effort we are undertaking is a major change, and it is refreshingly honest and appropriate that Act 48 obliges our lawmakers to identify a funding mechanism 4 full years in advance of its implementation—in 2013. This timing allows us to speak with legislative candidates in the coming election season and share our opinions on how our future health care should be funded.
Will the propaganda campaign succeed?
While the assertions of these propagandists are ridiculous, this does not mean that the propaganda campaign will fail. Reality doesn’t matter when the microphone available to the propagandists is so loud, and when the message the microphone is blaring is incessant. Prior propaganda campaigns have taught us that if you repeat a lie often enough, people will come to believe it.
And based on what we’ve seen in the last month, there appears to be no limit to the amount of money this organization has available to spew its disinformation. While many Vermonters may oppose or have doubts about the health reform effort, the scale and costliness of this media campaign make it quite unlikely that the campaign is funded within Vermont. My bet is that almost all of the funding is coming from pharmaceutical and health insurance companies. For these companies to spend all it takes to prevent single payer reform from succeeding—even in one state– is far less expensive in Vermont than it would be in most other states.
But we’ll never know. The key information that is being very consciously hidden from the public has nothing to do with what VHCF is alleging. What is being hidden from all of us is this question: Who is funding this propaganda campaign?
Green Mountain Care will bring all Vermonters into a system of health care they can access throughout their lives. And as is the case with single payer systems across the world, only this type of reform has the ability to control health care costs and provide care to every single citizen throughout their lives. The international track record is crystal clear: Single payer systems control costs, and they are very popular – far more popular than the nasty game of musical chairs that passes for a health care “system” here in the U.S.
But this reform threatens those powerful corporations who are quite content with the health care system just the way it is. And now we see them fighting back using the technique that usually works: Throwing unlimited amounts of money to create a propaganda offensive.
How can Vermonters respond?
1. Local media outlets should not air any media spots by organizations that refuse to disclose their funding sources
2. Local media outlets should provide airtime free of charge to local organizations and individuals who are able to provide sensible balance when such media campaigns support primarily the interests of well-funded corporate conglomerates whose media buys are orders of magnitude greater than what regular Vermonters could possibly afford.
3. If they are willing to air ads from such mysterious organizations, then local media outlets should severely limit the number of times the ads air so that they are not serving as passive conduits for disinformation campaigns. Effectively, they become complicit when they profit from propaganda that is harmful to the public interest.
4. If our local media outlets continue to serve as conduits for a propaganda campaign—and this definitely includes this case—then concerned citizens around the state should organize pickets and call-in campaigns directed at these stations. Media outlets have a duty to serve the public in an ethical and balanced manner. They need to respond appropriately to this new development in a manner that demonstrates their role of service to the public.
5. Host a public forum or public debate. Supporters of health reform are available around the state who are ready to speak publicly on the issue. I have personally offered to debate the opponents of reform in any suitable venue. I made this offer on WDEV’s Mark Johnson show last month—and Mark agreed to host such an event. Unsurprisingly, there has been no response so far.
Every Vermonter who wants to create an affordable and humane health care system for our state has a stake in this effort.
Marvin Malek, MD is a physician who practices internal medicine at Central Vermont Hospital.
http://vermontforsinglepayer.org/blog/2012/03/how-to-respond-to-the-%E2%80%9Chealth-care-freedom%E2%80%9D-propaganda-campaign/
By Marvin Malek, M.D.
Vermont for Single Payer, March 12, 2012
Vermonters are now being subjected to the most intense, well-funded propaganda campaign I have ever seen in Vermont.
Beginning in January of this year, the group, Vermonters for Health Care Freedom (VHCF), began to carpet bomb the airwaves with a media campaign targeting Act 48, the health reform law signed into law last May. The campaign uses the standard propaganda techniques of fear-mongering, distortion, and appeal to conspiracy theories.
Reality Check
The ads allege that a secret cabal of health reformers plan to raise our taxes by $5 billion to fund the new single payer system, that these conspirators already know how they plan to impose these taxes, and that they are hiding this information from the public.
Every element of this message is nonsense. Here’s the reality check:
$5 billion represents total health spending in Vermont currently. As is the case in most states, over half of Vermont’s health care money comes from federal sources. This includes funding for federal employees, the military, the VA, Medicare, and the majority of Medicaid funding. And Act 48, the reform bill, has been designed to ensure that we continue to receive all of the federal funding we normally receive. Furthermore, most of the remainder of the $5 billion is money we’re already raising. This encompasses out-of-pocket spending, health insurance premiums, and local and state taxes that are already funding health care for state and local employees, teachers, prisoners, VScript, Catamount, and Vermont’s portion of Medicaid spending.
So whatever additional revenue is required will represent only a small fraction of total health spending—not even close to $5 billion.
The ads never mention that Green Mountain Care—the proposed single payer plan– does not go into effect until 2017. Think about it: Is it realistic to expect those who are just beginning work on the reform effort to have already determined its entire funding structure—five years in advance? And that there is some sort of conspiracy related to Green Mountain Care’s funding for 2017? Next thing you know, they’ll claim a conspiracy if the Agency of Transportation or the Corrections Dept are unable to announce their 2017 budgets five years in advance.
Get real.
The truth is that the reform effort we are undertaking is a major change, and it is refreshingly honest and appropriate that Act 48 obliges our lawmakers to identify a funding mechanism 4 full years in advance of its implementation—in 2013. This timing allows us to speak with legislative candidates in the coming election season and share our opinions on how our future health care should be funded.
Will the propaganda campaign succeed?
While the assertions of these propagandists are ridiculous, this does not mean that the propaganda campaign will fail. Reality doesn’t matter when the microphone available to the propagandists is so loud, and when the message the microphone is blaring is incessant. Prior propaganda campaigns have taught us that if you repeat a lie often enough, people will come to believe it.
And based on what we’ve seen in the last month, there appears to be no limit to the amount of money this organization has available to spew its disinformation. While many Vermonters may oppose or have doubts about the health reform effort, the scale and costliness of this media campaign make it quite unlikely that the campaign is funded within Vermont. My bet is that almost all of the funding is coming from pharmaceutical and health insurance companies. For these companies to spend all it takes to prevent single payer reform from succeeding—even in one state– is far less expensive in Vermont than it would be in most other states.
But we’ll never know. The key information that is being very consciously hidden from the public has nothing to do with what VHCF is alleging. What is being hidden from all of us is this question: Who is funding this propaganda campaign?
Green Mountain Care will bring all Vermonters into a system of health care they can access throughout their lives. And as is the case with single payer systems across the world, only this type of reform has the ability to control health care costs and provide care to every single citizen throughout their lives. The international track record is crystal clear: Single payer systems control costs, and they are very popular – far more popular than the nasty game of musical chairs that passes for a health care “system” here in the U.S.
But this reform threatens those powerful corporations who are quite content with the health care system just the way it is. And now we see them fighting back using the technique that usually works: Throwing unlimited amounts of money to create a propaganda offensive.
How can Vermonters respond?
1. Local media outlets should not air any media spots by organizations that refuse to disclose their funding sources
2. Local media outlets should provide airtime free of charge to local organizations and individuals who are able to provide sensible balance when such media campaigns support primarily the interests of well-funded corporate conglomerates whose media buys are orders of magnitude greater than what regular Vermonters could possibly afford.
3. If they are willing to air ads from such mysterious organizations, then local media outlets should severely limit the number of times the ads air so that they are not serving as passive conduits for disinformation campaigns. Effectively, they become complicit when they profit from propaganda that is harmful to the public interest.
4. If our local media outlets continue to serve as conduits for a propaganda campaign—and this definitely includes this case—then concerned citizens around the state should organize pickets and call-in campaigns directed at these stations. Media outlets have a duty to serve the public in an ethical and balanced manner. They need to respond appropriately to this new development in a manner that demonstrates their role of service to the public.
5. Host a public forum or public debate. Supporters of health reform are available around the state who are ready to speak publicly on the issue. I have personally offered to debate the opponents of reform in any suitable venue. I made this offer on WDEV’s Mark Johnson show last month—and Mark agreed to host such an event. Unsurprisingly, there has been no response so far.
Every Vermonter who wants to create an affordable and humane health care system for our state has a stake in this effort.
Marvin Malek, MD is a physician who practices internal medicine at Central Vermont Hospital.
http://vermontforsinglepayer.org/blog/2012/03/how-to-respond-to-the-%E2%80%9Chealth-care-freedom%E2%80%9D-propaganda-campaign/
By Bill Toland
Pittsburgh Post-Gazette, March 14, 2012
One rationale behind the adoption of electronic medical records is that making a patient’s records more easily accessible for doctors will result in more efficient care, partly by reducing duplicative tests.
But physicians who have electronic systems — and, more crucially, have the ability to easily order X-rays, CT scans and MRI images via computer — are far more likely to order those kinds of tests than doctors without electronic access, according to a study published in the March issue of Health Affairs.
The results of the study run counter to the experts who believe electronic access to a patient’s medical history will ultimately improve the quality and efficiency of care.
So strong is that belief that the U.S. government, via the Health Information Technology for Economic and Clinical Health Act (or HITECH), has earmarked about $30 billion to be spent spurring health providers — primarily hospitals and physicians — to use information technology.
But the report — written by researchers from Harvard Medical School, the Cambridge Health Alliance and the school of public health at Hunter College — says that “physicians’ access to computerized imaging results was associated with a 40 to 70 percent greater likelihood of an imaging test being ordered.” Lab results also were ordered at a higher rate among the computerized cohort.
“We can only speculate about what’s behind our findings,” said David Himmelstein, health policy professor at Hunter College and one of the report’s co-authors. “The most likely explanation is, if you make it easier for doctors to get a test result, [they’re] going to say, ‘Might as well go ahead and order it.’ “
The study looked at 28,741 patient visits to nearly 1,200 office-based physicians in 2008. Physicians who did not have computerized access ordered imaging tests in 12.9 percent of visits; doctors with electronic access ordered imaging in 18 percent of visits. That’s a 40 percent increase in likelihood.
When it comes to advanced imaging, the “wired” doctors were about 70 percent more likely to order such tests than those without electronic access.
The study’s authors noted “these findings raise the possibility that, as currently implemented, electronic access does not decrease test ordering in the office setting and may even increase it, possibly because of system features that are enticements to ordering.”
While advocates of electronic records have said for decades that a paperless, wired health care system would help reduce errors and cost, and increase efficiency and outcomes, the data don’t always support those findings. In fact, the data sometimes supports the opposite — that electronic records, by themselves, don’t improve care.
“The people who make their living selling or programming computers [really] don’t like the results,” Mr. Himmelstein said. “There’s nothing approaching the type of solid evidence we demand of drugs or new medical devices that come on the market” when it comes to electronic records systems, he said.
Michael Furukawa, a health economist in the Office of the National Coordinator for Health Information Technology, told The Washington Post that the study “only looked at one piece of health IT. … The proper use of advanced health IT functions, we believe, will reduce costs in the long run.”
Mr. Himmelstein, as well as skeptics of electronic records in general, respond that it’s hard to know what entails “proper use” of advanced IT functions when the systems haven’t been vetted by an independent agency.
The HITECH act, which was part of the larger economic stimulus plan, was of “clear benefit to the economy … a lot of computer equipment got bought, and a lot of jobs were created,” Mr. Himmelstein said. But whether any of that spending is now benefiting patients, “We have no idea.”
In an ideal world, management would know if a software suite is going to improve health outcomes before it’s rolled out, said Nancy Finn, a medical consultant and author of “e-Patients Live Longer.” Unfortunately, though, uncertainty is built into the process.
“The only way to know [the systems] are inefficient and flawed is to deploy them, then correct them as we go,” she said.
“That is the way that all of the new innovative technologies have worked over the years. We have to take the risk, and then improvements get made. … Once the health records are in place for a longer period of time, [I] think you will begin to see a reduction in the numbers of these tests that are being ordered.”
http://www.post-gazette.com/stories/news/health/digital-ease-may-complicate-health-care-249299/?p=0
By Joe Jarvis
Utah Healthcare Initiative blog, March 10, 2012
Recently, Charles Krauthammer, conservative Washington Post commentator and Fox News analyst, who is also a physician, spoke to an audience of mostly physicians in San Antonio (find coverage of the speech in the San Antonio press here).
Excerpts from the article:
If President Barack Obama’s health care reform act is fully implemented over the next two years, it will evolve into a Canadian-style single-payer system that will forever change the social contract between Americans and their government, a nationally syndicated columnist and physician predicts.
“It will change the country. If it is not repealed, we will be a different country when ‘Obamacare’ is fully implemented,” Krauthammer said in an interview after speaking Thursday to a receptive crowd of mostly physicians and other health care professionals at a breakfast sponsored by the San Antonio Medical Foundation.
The Affordable Care Act, which passed in March 2010 without Republican support, was touted as a way to extend coverage to most uninsured Americans, and to offer it at an affordable price to those who have trouble buying it now, such as the poor, the self-employed, and those with pre-existing medical conditions.
The centerpiece of the plan is a requirement for everyone without health coverage to buy a policy or pay a fine. Krauthammer predicted that the U.S. Supreme Court, which is set to deliberate the constitutionality of the Affordable Care Act this month, will overturn the that provision of the law.
“The individual mandate (to buy health insurance) is a fairly radical step in the final expansion of the power of the federal government, which would then leave it in a position where it would be very hard to find any constitutional grounds — if you don’t overturn this — for ever denying the federal government the power to do anything it wants,” Krauthammer said.
“We’re spending perhaps $1 out of every $4 on unnecessary treatments, referrals and tests that everyone knows are unnecessary,” he said. “And Obamacare did nothing to reform it.”
In his speech, Krauthammer predicted the complexity of the law eventually would doom it to failure, which would lead to a single-payer system within a decade.
“This is a new reform that when it kicks in within a couple of years will make the practice of medicine a nightmare,” he said. “If it’s not repealed, I guarantee you that within a decade we will have a single-payer system. And if I had to choose between Obamacare and a Canadian or British system, I’d choose the single-payer system. At least it would be rational.”
My comment:
It’s clear from his comments that Dr. Krauthammer wishes that Obamacare would be repealed and that the nation would not go down the pathway towards single-payer health system reform. However, he directly states that given a choice between Obamacare and single payer, he would choose single payer, because “at least it would be rational.”
What does a conservative like Krauthammer see in single-payer health system reform that is rational? I feel qualified to answer that question, since I am both a conservative (I received the Republican nomination twice for legislative races in Salt Lake City) and a longtime support of single-payer health system reform.
First, and foremost from a conservative viewpoint, single-payer health system reform is fiscally responsible. Unlike the ‘Affordable’ Care Act, a single-payer approach to health system financing is financially sustainable. Nearly all of the unfunded future debt due to entitlements currently stacked up against the federal government is medical debt. The last count for that debt which I have seen is $60 trillion, more than the present day value of all assets owned in the U.S. Single-payer health system reform can reduce the cost of health care by $1 trillion/year, nearly all of which can go to relieving the tax burden. By the time today’s kindergartners are Medicare eligible, a single-payer-style payment mechanism for American health care would have eliminated the federal deficit.
Second, and integral to cost control, single-payer health system reform has the capability to eliminate the poor quality care due to unnecessary treatments. Eliminating the multiple, confusing payment schemes for health services also eliminates the perverse incentives inherent in those schemes. The health insurance business model induces provider behaviors which are contrary to good patient care. In contrast, single-payer health financing focuses providers on best practices for patient care. It is, as Krauthammer notes, the most rational method of paying for health care.
Third, single-payer health system reform can (and should) be implemented at the state level, preserving the appropriate balance between national and local governing.
I disagree with Dr. Krauthammer. Obamacare does not make single-payer health system reform inevitable. If we Americans want a health system that is optimal quality and therefore lowest cost, we will have to do the heavy political lifting necessary to intentionally rid our health system of corporate welfare, clearing the decks for a rational payment mechanism which cherishes patient care above profits. It’s the most conservative way forward for our health care system.
http://utahhealthcareinitiative.com/blog/conservative-case-single-payer-health-reform
By Therese A. Stukel, PhD; Elliott S. Fisher, MD, MPH; David A. Alter, MD, PhD; Astrid Guttmann, MD, MSc; Dennis T. Ko, MD, MSc; Kinwah Fung, MSc; Walter P. Wodchis, PhD; Nancy N. Baxter, MD, PhD; Craig C. Earle, MD, MSc; Douglas S. Lee, MD, PhD
JAMA, March 14, 2012
The extent to which better spending produces higher-quality care and better patient outcomes in a universal health care system with selective access to medical technology is unknown.
Numerous studies have investigated whether higher health care spending produces better patient outcomes and higher quality of care. Evidence from the United States and other countries has been conflicting. Several studies focusing on short-term outcomes within a given state found that being treated in higher-spending hospitals was associated with better in-hospital or 30-day mortality. In contrast, a national study found that regional differences in spending intensity were largely attributable to use of the hospital as a site of care and greater overall use of specialists, imaging, and diagnostic testing but that patients treated in regions with higher spending intensity did not have better survival or quality of care. Whether these findings would hold true in a country with universal access to health care but a far lower supply of specialists and more selective access to medical technology is unknown.
Our objective was to assess whether acute care patients admitted to Canadian hospitals that treat patients more intensively (and at higher cost) have lower mortality and readmissions and higher quality of care.
We found that higher hospital spending intensity was associated with better survival, lower readmission rates, and better quality of care for seriously ill, hospitalized patients in Ontario in a universal health care system with more selective access to medical technology. Higher-spending hospitals were higher-volume teaching or community hospitals with high-volume or specialist attending physicians and having specialized programs, such as regional cancer centers, and specialized services, such as on-site cardiac catheterization, cardiac surgery, and diagnostic imaging facilities. The study also points to plausible mechanisms through which higher spending may be associated with better outcomes.
Benefits appeared early, suggesting an acute-phase hospital effect. For acute conditions, timely access to preoperative and in-hospital specialist care, skilled nursing staff, rapid response teams, cardiac high-technology services, and regional cancer centers, all found in the higher-spending systems, are related to better outcomes. These systems also provided consistently, but not strikingly, higher levels of evidence-based care and collaborative ambulatory care, both shown to improve care. Higher spending on evidence-based services delivered in the acute phase of care for severely ill hospitalized patients—by far the largest component of spending for our cohorts—is indeed likely to be beneficial.
To place the study in context, the United States has a 3- to 4-times higher per capita supply of specialized technology, such as computed tomography and magnetic resonance imaging scanners, but a similar supply of acute care beds and nurses. Ontario 2001 population rates of cardiac testing and revascularization lagged behind corresponding 1992 US rates and paralleled the supply of cardiologists and catheterization facilities. It is therefore possible that Canadian hospitals, with fewer specialized resources, selective access to medical technology, and global budgets, are using these resources more efficiently, especially during the inpatient episode for care-sensitive conditions. Canada’s health care expenditures per capita are about 57% of those in the United States. At this spending level, there might still be a positive association between spending and outcomes.
We cannot rule out the possibility that higher-intensity hospitals coded more aggressively, but there is less incentive to do so in a system with global hospital budgets.
This study shows that in Ontario, a province with global hospital budgets and fewer specialized health care resources than the United States, outcomes following an acute hospitalization are positively associated with higher hospital spending intensity. Higher spending intensity, in turn, is associated with greater use of specialists, better patient care, and more use of advanced procedures. These results suggest that it is critical to understand not simply how much money is spent but whether it is spent on effective procedures and services.
http://jama.ama-assn.org/content/307/10/1037.abstract
eAppendix – to article above (15 pages):
Costing Data Sources
The following is an excerpt from Guidelines on Person-Level Costing Using Administrative Databases in Ontario that describes the costing methodology for acute inpatient hospitalizations, emergency visits (ED), and physician services, based on Ontario healthcare utilization data. Total costs (direct costs and overheads) for acute care and ED are available from the Ontario Ministry of Health and Long-Term Care (MOHLTC) Health Data Branch and are based on Ontario Cost Distribution Methodology (OCDM). Fees associated with physician visits are available directly from the Ontario Health Insurance Plan (OHIP) Schedule of Claims and Benefits while fees paid to physicians are tracked in the OHIP physician billing database.
http://jama.ama-assn.org/content/suppl/2012/03/07/307.10.1037.DC1/JWE20016_03_14_2012.pdf
And…
By Karen E. Joynt, MD, MPH; Ashish K. Jha, MD, MPH
JAMA, March 14, 2012
Editorial
For the past 30 years, research from investigators at Dartmouth has demonstrated large and persistent variations in costs and quality across the US health care system. Beyond simply showing that cost and quality vary by geography, the Dartmouth Atlas has demonstrated that in many communities, care is so fragmented and ineffective that greater spending on Medicare beneficiaries often leads to worse outcomes because some patients receive services that are redundant and low value and that may even have substantial risks.
However, some US policy makers have misinterpreted the Dartmouth research and in the troves of data have found what they believe to be a free lunch: given the inverse relationship between costs and quality, it follows that it should be possible to simultaneously reduce spending and improve care. Although this notion is attractive, much of the subtlety of the Dartmouth work has been lost in translation. What Dartmouth investigators have documented through careful work is that dysfunctional systems produce expensive, poor-quality care.
Data from Dartmouth researchers and others have thus led policy makers to feel comfortable with broad payment reductions, in many cases targeting hospitals as a major source of savings for the Medicare program. The Affordable Care Act requires that the Centers for Medicare & Medicaid Services (CMS) make a series of payment reductions to hospitals, and CMS has proposed other reductions. Nearly every proposal to reduce Medicare spending, from Democrats and Republicans alike, seems to contain reductions in Medicare payments to hospitals. The notion that payments to hospitals can be reduced while maintaining or improving the quality of care delivered at these hospitals has become so ingrained in policy circles as to be a given.
Recently, however, an increasing amount of evidence has em
erged that should counter this misperception. Several studies suggest that higher spending at the patient or hospital level may in fact be associated with better clinical outcomes.
What are federal policy makers to do? One lesson is that although broad-based reductions in hospital reimbursement may spur some institutions to innovate and eliminate waste, others will surely cut costs indiscriminately, eliminating exactly those services that are vital for good hospital care. Given that many hospitals may not have a clear sense of how to make these reductions without compromising on important services and personnel, patients will likely be negatively affected. An alternative approach is to target poor coordination, wasteful spending, and ineffective care more directly through programs such as bundled payments and accountable care organizations, which encourage coordination and integration first and spending reductions second. Ultimately, the best way to save money on hospital care is to more aggressively target preventable hospitalizations by bolstering primary care. These kinds of efforts are more likely to be successful in eliminating waste without jeopardizing patient outcomes. Although paying hospitals less may appear to be a good strategy to save money, the findings reported by Stukel et al serve as a timely reminder that this approach is likely to have negative consequences for patients.
http://jama.ama-assn.org/content/307/10/1082.full?etoc
By Don McCanne, MD
This is a landmark study. Among Ontario hospitals, higher spending intensity was associated with lower mortality, readmissions, and cardiac event rates. Let’s see if we can learn the right policy lessons from this.
With our very high levels of health care spending, yet mediocre quality and outcomes, attention has been directed to attempting to identify the basis of these discrepancies, especially by looking at the Dartmouth findings which have suggested that all too frequently there is no relationship or perhaps even an inverse relationship between greater spending in hospitals and high quality outcomes. This task has been made difficult by the fact that several other studies have shown that greater spending has improved outcomes.
The authors of this new study decided to look at hospitals in Ontario, Canada to try to identify more precisely whether or not increased spending does improve quality and outcomes. Although they didn’t state this as a reason, this was an astute move since Canadian hospitals are globally budgeted – a fact that dramatically reduces the incentives to increase the intensity of services for the purpose of increasing revenues. Attention is given to using resources to benefit the patient, without the perverse motive of increasing income by adding services of negligible or negative value.
In this environment, it worked. If patients needed more care, they got it, and they were better off for it. Incidentally, even with this extra care, they spent much less per patient than we do in the United States.
In the JAMA editorial accompanying this article, the authors indicate that this confirms further that there is “no free lunch” in trying to recover higher costs while improving quality. They suggest a few policy lessons.
Of great importance, efforts to reduce spending in high cost hospitals should not be indiscriminate since that risks eliminating “exactly those services that are vital for good hospital care.” Such reductions can negatively affect patients.
They suggest targeting “poor coordination, wasteful spending, and ineffective care more directly through programs such as bundled payments and accountable care organizations, which encourage coordination and integration first and spending reductions second.” Integrated, coordinated care is a great idea, and likely accounts for much of the improved outcomes in Ontario hospitals. But can we in the United States really achieve this through bundled payments and accountable care organizations?
Only certain clinical scenarios are subject to bundling. Even when bundled, the cost containment is achieved by providing a discount to the bundled package. Not only are there pricing issues, such as possible inadequate funding of the services, there is the much greater problem that this does nothing for total global spending. It more likely results in not much more than mere cost shifting. That won’t correct the fundamental dysfunctions in U.S. health care financing.
Much has been written about accountable care organizations. Unfortunately, as they are evolving, it looks like they won’t be much more than a replay of managed care innovations such as physician-hospital organizations, or loose provider networks under an HMO umbrella – except all dressed up in new clothing. It is particularly difficult to understand how the organization can be accountable for the care of the patient, when that patient is free to obtain care anywhere and may not even be aware that they are assigned to one organization. Again, integration and coordination are great, but that should occur throughout the medical community at large rather than through isolated, commercialized entities.
A most important policy lesson advanced by the editorialists is that “the best way to save money on hospital care is to more aggressively target preventable hospitalizations by bolstering primary care.” In fact, Canada has a much more robust primary care infrastructure than the United States, which is likely another contributor to getting the right patients into the Ontario hospitals at the right time. We need to do much more to reinforce primary care in the U.S. – far more than the meager measures in the Affordable Care Act.
The paramount take home policy lesson is that a single payer system such as that in Canada not only has vastly superior methods of financing and distributing health care resources efficiently and equitably, it also creates a milieu in which the patient is placed at the pinnacle, and the health care system is positioned to serve that patient optimally.
Association of Hospital Spending Intensity With Mortality and Readmission Rates in Ontario Hospitals
By Therese A. Stukel, PhD; Elliott S. Fisher, MD, MPH; David A. Alter, MD, PhD; Astrid Guttmann, MD, MSc; Dennis T. Ko, MD, MSc; Kinwah Fung, MSc; Walter P. Wodchis, PhD; Nancy N. Baxter, MD, PhD; Craig C. Earle, MD, MSc; Douglas S. Lee, MD, PhD
JAMA, March 14, 2012
The extent to which better spending produces higher-quality care and better patient outcomes in a universal health care system with selective access to medical technology is unknown.
Numerous studies have investigated whether higher health care spending produces better patient outcomes and higher quality of care. Evidence from the United States and other countries has been conflicting. Several studies focusing on short-term outcomes within a given state found that being treated in higher-spending hospitals was associated with better in-hospital or 30-day mortality. In contrast, a national study found that regional differences in spending intensity were largely attributable to use of the hospital as a site of care and greater overall use of specialists, imaging, and diagnostic testing but that patients treated in regions with higher spending intensity did not have better survival or quality of care. Whether these findings would hold true in a country with universal access to health care but a far lower supply of specialists and more selective access to medical technology is unknown.
Our objective was to assess whether acute care patients admitted to Canadian hospitals that treat patients more intensively (and at higher cost) have lower mortality and readmissions and higher quality of care.
We found that higher hospital spending intensity was associated with better survival, lower readmission rates, and better quality of care for seriously ill, hospitalized patients in Ontario in a universal health care system with more selective access to medical technology. Higher-spending hospitals were higher-volume teaching or community hospitals with high-volume or specialist attending physicians and having specialized programs, such as regional cancer centers, and specialized services, such as on-site cardiac catheterization, cardiac surgery, and diagnostic imaging facilities. The study also points to plausible mechanisms through which higher spending may be associated with better outcomes.
Benefits appeared early, suggesting an acute-phase hospital effect. For acute conditions, timely access to preoperative and in-hospital specialist care, skilled nursing staff, rapid response teams, cardiac high-technology services, and regional cancer centers, all found in the higher-spending systems, are related to better outcomes. These systems also provided consistently, but not strikingly, higher levels of evidence-based care and collaborative ambulatory care, both shown to improve care. Higher spending on evidence-based services delivered in the acute phase of care for severely ill hospitalized patients—by far the largest component of spending for our cohorts—is indeed likely to be beneficial.
To place the study in context, the United States has a 3- to 4-times higher per capita supply of specialized technology, such as computed tomography and magnetic resonance imaging scanners, but a similar supply of acute care beds and nurses. Ontario 2001 population rates of cardiac testing and revascularization lagged behind corresponding 1992 US rates and paralleled the supply of cardiologists and catheterization facilities. It is therefore possible that Canadian hospitals, with fewer specialized resources, selective access to medical technology, and global budgets, are using these resources more efficiently, especially during the inpatient episode for care-sensitive conditions. Canada’s health care expenditures per capita are about 57% of those in the United States. At this spending level, there might still be a positive association between spending and outcomes.
We cannot rule out the possibility that higher-intensity hospitals coded more aggressively, but there is less incentive to do so in a system with global hospital budgets.
This study shows that in Ontario, a province with global hospital budgets and fewer specialized health care resources than the United States, outcomes following an acute hospitalization are positively associated with higher hospital spending intensity. Higher spending intensity, in turn, is associated with greater use of specialists, better patient care, and more use of advanced procedures. These results suggest that it is critical to understand not simply how much money is spent but whether it is spent on effective procedures and services.
http://jama.ama-assn.org/content/307/10/1037.abstract
eAppendix – to article above (15 pages):
Costing Data Sources
The following is an excerpt from Guidelines on Person-Level Costing Using Administrative Databases in Ontario that describes the costing methodology for acute inpatient hospitalizations, emergency visits (ED), and physician services, based on Ontario healthcare utilization data. Total costs (direct costs and overheads) for acute care and ED are available from the Ontario Ministry of Health and Long-Term Care (MOHLTC) Health Data Branch and are based on Ontario Cost Distribution Methodology (OCDM). Fees associated with physician visits are available directly from the Ontario Health Insurance Plan (OHIP) Schedule of Claims and Benefits while fees paid to physicians are tracked in the OHIP physician billing database.
http://jama.ama-assn.org/content/suppl/2012/03/07/307.10.1037.DC1/JWE20016_03_14_2012.pdf
And…
No Free Lunch: The Relationship Between Cost and Quality
By Karen E. Joynt, MD, MPH; Ashish K. Jha, MD, MPH
JAMA, March 14, 2012
Editorial
For the past 30 years, research from investigators at Dartmouth has demonstrated large and persistent variations in costs and quality across the US health care system. Beyond simply showing that cost and quality vary by geography, the Dartmouth Atlas has demonstrated that in many communities, care is so fragmented and ineffective that greater spending on Medicare beneficiaries often leads to worse outcomes because some patients receive services that are redundant and low value and that may even have substantial risks.
However, some US policy makers have misinterpreted the Dartmouth research and in the troves of data have found what they believe to be a free lunch: given the inverse relationship between costs and quality, it follows that it should be possible to simultaneously reduce spending and improve care. Although this notion is attractive, much of the subtlety of the Dartmouth work has been lost in translation. What Dartmouth investigators have documented through careful work is that dysfunctional systems produce expensive, poor-quality care.
Data from Dartmouth researchers and others have thus led policy makers to feel comfortable with broad payment reductions, in many cases targeting hospitals as a major source of savings for the Medicare program. The Affordable Care Act requires that the Centers for Medicare & Medicaid Services (CMS) make a series of payment reductions to hospitals, and CMS has proposed other reductions. Nearly every proposal to reduce Medicare spending, from Democrats and Republicans alike, seems to contain reductions in Medicare payments to hospitals. The notion that payments to hospitals can be reduced while maintaining or improving the quality of care delivered at these hospitals has become so ingrained in policy circles as to be a given.
Recently, however, an increasing amount of evidence has emerged that should counter this misperception. Several studies suggest that higher spending at the patient or hospital level may in fact be associated with better clinical outcomes.
What are federal policy makers to do? One lesson is that although broad-based reductions in hospital reimbursement may spur some institutions to innovate and eliminate waste, others will surely cut costs indiscriminately, eliminating exactly those services that are vital for good hospital care. Given that many hospitals may not have a clear sense of how to make these reductions without compromising on important services and personnel, patients will likely be negatively affected. An alternative approach is to target poor coordination, wasteful spending, and ineffective care more directly through programs such as bundled payments and accountable care organizations, which encourage coordination and integration first and spending reductions second. Ultimately, the best way to save money on hospital care is to more aggressively target preventable hospitalizations by bolstering primary care. These kinds of efforts are more likely to be successful in eliminating waste without jeopardizing patient outcomes. Although paying hospitals less may appear to be a good strategy to save money, the findings reported by Stukel et al serve as a timely reminder that this approach is likely to have negative consequences for patients.
http://jama.ama-assn.org/content/307/10/1082.full?etoc
This is a landmark study. Among Ontario hospitals, higher spending intensity was associated with lower mortality, readmissions, and cardiac event rates. Let’s see if we can learn the right policy lessons from this.
With our very high levels of health care spending, yet mediocre quality and outcomes, attention has been directed to attempting to identify the basis of these discrepancies, especially by looking at the Dartmouth findings which have suggested that all too frequently there is no relationship or perhaps even an inverse relationship between greater spending in hospitals and high quality outcomes. This task has been made difficult by the fact that several other studies have shown that greater spending has improved outcomes.
The authors of this new study decided to look at hospitals in Ontario, Canada to try to identify more precisely whether or not increased spending does improve quality and outcomes. Although they didn’t state this as a reason, this was an astute move since Canadian hospitals are globally budgeted – a fact that dramatically reduces the incentives to increase the intensity of services for the purpose of increasing revenues. Attention is given to using resources to benefit the patient, without the perverse motive of increasing income by adding services of negligible or negative value.
In this environment, it worked. If patients needed more care, they got it, and they were better off for it. Incidentally, even with this extra care, they spent much less per patient than we do in the United States.
In the JAMA editorial accompanying this article, the authors indicate that this confirms further that there is “no free lunch” in trying to recover higher costs while improving quality. They suggest a few policy lessons.
Of great importance, efforts to reduce spending in high cost hospitals should not be indiscriminate since that risks eliminating “exactly those services that are vital for good hospital care.” Such reductions can negatively affect patients.
They suggest targeting “poor coordination, wasteful spending, and ineffective care more directly through programs such as bundled payments and accountable care organizations, which encourage coordination and integration first and spending reductions second.” Integrated, coordinated care is a great idea, and likely accounts for much of the improved outcomes in Ontario hospitals. But can we in the United States really achieve this through bundled payments and accountable care organizations?
Only certain clinical scenarios are subject to bundling. Even when bundled, the cost containment is achieved by providing a discount to the bundled package. Not only are there pricing issues, such as possible inadequate funding of the services, there is the much greater problem that this does nothing for total global spending. It more likely results in not much more than mere cost shifting. That won’t correct the fundamental dysfunctions in U.S. health care financing.
Much has been written about accountable care organizations. Unfortunately, as they are evolving, it looks like they won’t be much more than a replay of managed care innovations such as physician-hospital organizations, or loose provider networks under an HMO umbrella – except all dressed up in new clothing. It is particularly difficult to understand how the organization can be accountable for the care of the patient, when that patient is free to obtain care anywhere and may not even be aware that they are assigned to one organization. Again, integration and coordination are great, but that should occur throughout the medical community at large rather than through isolated, commercialized entities.
A most important policy lesson advanced by the editorialists is that “the best way to save money on hospital care is to more aggressively target preventable hospitalizations by bolstering primary care.” In fact, Canada has a much more robust primary care infrastructure than the United States, which is likely another contributor to getting the right patients into the Ontario hospitals at the right time. We need to do much more to reinforce primary care in the U.S. – far more than the meager measures in the Affordable Care Act.
The paramount take home policy lesson is that a single payer system such as that in Canada not only has vastly superior methods of financing and distributing health care resources efficiently and equitably, it also creates a milieu in which the patient is placed at the pinnacle, and the health care system is positioned to serve that patient optimally.
Congressional Budget Office
March 2012
In preparing the March 2012 baseline budget projections, the Congressional Budget Office (CBO) and the staff of the Joint Committee on Taxation (JCT) have updated estimates of the budgetary effects of the health insurance coverage provisions of the Affordable Care Act (ACA).
CBO and JCT now estimate that the insurance coverage provisions of the ACA will have a net cost of just under $1.1 trillion over the 2012–2021 period — about $50 billion less than the agencies’ March 2011 estimate for that 10-year period.
CBO and JCT’s projections of health insurance coverage have also changed since last March. Fewer people are now expected to obtain health insurance coverage from their employer or in insurance exchanges; more are now expected to obtain coverage from Medicaid or CHIP or from nongroup or other sources. More are expected to be uninsured.
Compared with prior law, the ACA is now estimated by CBO and JCT to reduce the number of nonelderly people without health insurance coverage by 30 million to 33 million in 2016 and subsequent years, leaving 26 million to 27 million nonelderly residents uninsured in those years.
http://www.cbo.gov/system/assets/drupal/cbofiles/attachments/03-13-Coverage%20Estimates.pdf
By Don MCCanne, MD
So the projected federal spending on the Affordable Care Act over the next decade will be $50 billion less than previous projections. Directing attention to that flimsy fact hides the real news in this report. Instead of 23 million individuals being left uninsured, as the CBO previously predicted, it is now estimated that 26 to 27 million will have no insurance at all.
These numbers are approaching the 34.7 million uninsured in 1990 – a time when health reform was pushing its way back to the top of the political agenda. It was a national disgrace that we had allowed ourselves to become world leaders in both health care spending and health care injustice!
So now we finally have passed health reform legislation, but what have we actually accomplished? Higher costs, deterioration in the protection afforded by insurance, and projected uninsured rates close to those when we began this whole process.
Wasting the next decade or two tinkering with the Affordable Care Act, pretending that we’re making real progress, just won’t cut it. There are no adequate policies in the ACA model on which to build substantial reform. We need truly efficacious reform that covers absolutely everyone equitably in a universal program – a single payer national health program.
Every year that goes by without acting brings us ever more health care tragedies, not to mention financial hardship. We can’t wait around while we watch the unfolding of the failure of the ACA experiment. We need reform now. It’s an absolute moral imperative!
Updated Estimates for the Insurance Coverage Provisions of the Affordable Care Act
Congressional Budget Office
March 2012
In preparing the March 2012 baseline budget projections, the Congressional Budget Office (CBO) and the staff of the Joint Committee on Taxation (JCT) have updated estimates of the budgetary effects of the health insurance coverage provisions of the Affordable Care Act (ACA).
CBO and JCT now estimate that the insurance coverage provisions of the ACA will have a net cost of just under $1.1 trillion over the 2012–2021 period — about $50 billion less than the agencies’ March 2011 estimate for that 10-year period.
CBO and JCT’s projections of health insurance coverage have also changed since last March. Fewer people are now expected to obtain health insurance coverage from their employer or in insurance exchanges; more are now expected to obtain coverage from Medicaid or CHIP or from nongroup or other sources. More are expected to be uninsured.
Compared with prior law, the ACA is now estimated by CBO and JCT to reduce the number of nonelderly people without health insurance coverage by 30 million to 33 million in 2016 and subsequent years, leaving 26 million to 27 million nonelderly residents uninsured in those years.
http://www.cbo.gov/system/assets/drupal/cbofiles/attachments/03-13-Coverage%20Estimates.pdf
So the projected federal spending on the Affordable Care Act over the next decade will be $50 billion less than previous projections. Directing attention to that flimsy fact hides the real news in this report. Instead of 23 million individuals being left uninsured, as the CBO previously predicted, it is now estimated that 26 to 27 million will have no insurance at all.
These numbers are approaching the 34.7 million uninsured in 1990 – a time when health reform was pushing its way back to the top of the political agenda. It was a national disgrace that we had allowed ourselves to become world leaders in both health care spending and health care injustice!
So now we finally have passed health reform legislation, but what have we actually accomplished? Higher costs, deterioration in the protection afforded by insurance, and projected uninsured rates close to those when we began this whole process.
Wasting the next decade or two tinkering with the Affordable Care Act, pretending that we’re making real progress, just won’t cut it. There are no adequate policies in the ACA model on which to build substantial reform. We need truly efficacious reform that covers absolutely everyone equitably in a universal program – a single payer national health program.
Every year that goes by without acting brings us ever more health care tragedies, not to mention financial hardship. We can’t wait around while we watch the unfolding of the failure of the ACA experiment. We need reform now. It’s an absolute moral imperative!
By Danny McCormick, David Bor, Stephanie Woolhandler, and David Himmelstein
Health Affairs Blog, March 12th, 2012
Our recent Health Affairs article linking increased test ordering to electronic access to results has elicited heated responses, including a blog post by Farzad Mostashari, National Coordinator for Health IT. Some of the assertions in his blog post are mistaken. Some take us to task for claims we never made, or for studying only some of the myriad issues relevant to medical computing. And many reflect wishful thinking regarding health IT; an acceptance of deeply flawed evidence of its benefit, and skepticism about solid data that leads to unwelcome conclusions.
Dr. Mostashari’s use of a government website to critique our paper, will, we hope, open a fruitful dialogue. We trust that in the interest of fairness he will also post our response on his agency’s site.
Our study analyzed government survey data on a nationally representative sample of 28,741 patient visits to 1187 office-based physicians. We found that electronic access to computerized imaging results (either the report or the actual image) was associated with a 40% -70% increase in imaging tests, including sharp increases in expensive tests like MRIs and CT scans; the findings for blood tests were similar. Although the survey did not collect data on payments for the tests, it’s hard to imagine how a 40% to 70% increase in testing could fail to increase imaging costs.
Dr. Mostashari’s statement that “reducing test orders is not the way that health IT is meant to reduce costs” is surprising, and contradicts statements by his predecessor as National Coordinator that electronic access to a previous CT scan helped him to avoid ordering a duplicate and “saved a whole bunch of money.” A Rand study, widely cited by health IT advocates including President Obama, estimated that health IT would save $6.6 billion annually on outpatient imaging and lab testing. Another frequently quoted estimate of HIT-based savings projected annual cost reductions of $8.3 billion on imaging and $8.1 billion on lab testing.
We focused on electronic access to results because the common understanding of how health IT might decrease test ordering is that it would facilitate retrieval of previous results, avoiding duplicate tests. Indeed, it’s clear from the extensive press coverage that our study was seen as contravening this “conventional wisdom”.
Nonetheless, Dr. Mostashari criticizes us for analyzing the impact of physicians’ electronic access to imaging and test results, but not other aspects of electronic health record (EHR) use. We did, however, analyze the relationship of EHRs to test ordering in a subsidiary analysis. While physicians use of a full EHR was associated with a 19% increase in image ordering, as we noted in the paper this finding was not statistically significant. While we cautiously (and properly) interpreted this as a “null” finding, these data are inconsistent with Mostashari’s optimistic view that use of a full EHR reduces costs.
He asserts that our 2008 data are passe, and that health IT meeting today’s “meaningful use” criteria definitely saves money. The data we analyzed were the latest available data when we initiated the study. While the proportion of outpatient physicians utilizing health IT has grown since 2008, we are unaware of any “game changing” health IT developments in the past four years that are would produce substantially different results if the study were repeated today. The EHR vendors that dominated the market in 2008 remain, by and large, today’s market leaders, and their products have undergone mostly modest tweaks. Mostashari’s contention that 2012 EHRs – incorporating decision support and electronic information exchange – save money in ways not possible in 2008 should be tested through additional research but remains merely a hypothesis. We hope that some day his predicted savings can be achieved.
Dr. Mostashari offers his own explanation for our findings, suggesting that doctors who are inclined to order more tests are also inclined to purchase health IT for viewing test results electronically rather than on paper. He offers no evidence for this assertion and ignores the fact that we explored (and rejected) this explanation by analyzing subgroups of doctors who are unlikely to be the decision maker for IT purchases – e.g. employed physicians, those working in an HMO setting etc. In other words, electronic access to results predicted more test ordering whether or not the ordering physician was responsible for health IT purchases.
He incorrectly states that our analysis did not take into account patients’ severity of illness, physicians’ level of training, and the nature of physicians’ financial arrangements. In fact, we reported subsidiary multivariate analyses that included several serious diagnoses; all of our models included physician specialty (which we specified in several different ways); and all models included adjustment for an extensive list of indicators of financial arrangements (e.g. whether the physician owned the practice or was an employee; the type of office; whether the practice was owned by a hospital; whether the physician was a solo practitioner; whether the physician’s compensation was based, in part or whole on “profiling”; and whether the practice was predominantly prepaid). We also performed a series of subsidiary analyses that explored whether physicians with a proclivity to “self refer” patients for imaging tests accounted for our finding; they didn’t.
Dr. Mostashari criticizes us for failing to assess whether health IT improved the quality or appropriateness of care. Of course, these were not the topic of our research. Those are different studies for a different time. However, we would note that other large-scale studies have found no, or trivial quality improvements associated with HIT outside of a few flagship institutions4-6.
Dr. Mostashari’s strongest claim is that observational studies like ours (and most other health policy studies, including some by Dr. Mostashari himself) cannot prove causation. This is surely true. As long time teachers of evidence based medicine we took care to couch our conclusions in cautious terms, stating only that “Computerization, whatever its other benefits, remains unproven as a cost control strategy.”
But Dr. Motashari is less cautious, asserting that the case for HIT is closed. The paper he cites to buttress this claim (authored by members of his own agency) culled studies reporting any impact of HIT on virtually any aspect of care, and accepted authors’ claims of benefit without regard to study quality or statistical niceties. Thus, a focus group’s impressions of benefit are accorded the same weight as nationwide studies of Medicare data showing virtually no impact of computerization on quality measures. Reports of a reduction from 70% to 38 % in “missed bi
lling opportunities” or a $7,000 reduction in office supply costs are among the 92% of studies judged “positive”. While the literature review he cites is interesting, nothing in it contradicts our findings.
Dr. Mostashari is also correct in reiterating that randomized trials are the best way to assess health IT. In fact, no randomized trial has ever been published that examines patients’ outcomes or costs associated with off-the-shelf health IT systems that dominate the U.S. market. No drug or new medical device could pass FDA review based on such thin evidence as we have on health IT. Yet his agency is disbursing $19 billion in federal funds to stimulate the adoption of this inadequately evaluated technology. Dr. Mostashari is perhaps the only person in our nation who commands the resources needed to mount a well done randomized controlled trial to fairly assess the impact of health IT, and the comparative efficacy of the various EHR options.
Finally, Dr. Mostashari’s unbridled faith in technology is mirrored by his belief that ACOs are the next panacea for health costs and quality. That health policy flavor-of-the-month also remains wholly unproven.
Department of Health and Human Services
Federal Register publication date: March 27, 2012
Final rule, Interim final rule.
Excerpts from pages 34-37
Summary of Regulatory Changes
If the Exchange is an independent State agency or not-for-profit entity established by the State, we proposed that its governing board meet the standards outlined in §155.110(c)(1) through §155.110(c)(4) of the proposed rule, which included: the Exchange accountability structure must be administered under a formal, publicly-adopted operating charter or by-laws; the Exchange board must hold regular public meetings; representatives of health insurance issuers, agents, brokers, or other individuals licensed to sell health insurance may not constitute a majority of the governing board; and, all members of the governing board must meet conflict of interest and qualifications standards.
Several commenters urged HHS to apply conflict of interest standards to eligible contracting entities.
Response: We generally defer to States to establish conflict of interest standards for eligible contracting entities beyond the prohibition of health insurance issuers being eligible contracting entities, as established in section 1311(f)(3) of the Affordable Care Act and codified in §155.110(a)(1)(iii). We believe that many States have existing conflict of interest laws, have appropriate expertise in this area, and can support Exchanges in the development of conflict of interest standards for such entities.
Commenters suggested broadening the list of groups identified as having a conflict of interest in proposed §155.110(c)(3)(ii) to include: health care providers; anyone with a financial interest; anyone with a spouse or immediate family with a conflict of interest; major vendors, subcontractors, or other financial partners of conflicted parties; members of health trade associations and providers; and, health information technology companies. Commenters recommended that such groups be limited or prohibited from participation in an Exchange. Other commenters recommended that individuals with ties to the insurance industry participate through technical panel or advisory group instead of through board membership.
Response: As proposed, §155.110(c)(3)(ii) ensures as a minimum standard that the groups with the most direct conflict of interest cannot form a majority of voting members on a governing board. We believe that further definition of conflict of interest may create inconsistencies with State law and other existing State standards, but note that Exchanges may expand the list or further define conflict of interest. For example, a State may elect to prohibit any conflicted members from serving on the board.
Final rule, Interim final rule. (644 pages):
http://www.kaiserhealthnews.org/~/media/Files/2012/Exchange%20Standards%20For%20Employers%20March%202012.pdf
HHS release:
http://www.healthcare.gov/news/factsheets/2011/07/exchanges07112011a.html
Reulatory impact analysis:
http://www.kaiserhealthnews.org/~/media/Files/2012/Exchange%20Regulatory%20Impact%20Analysis%20March%202012.pdf
By Don McCanne, MD
Skim reading this 644 page HHS rule on the state insurance exchanges to be established under the Affordable Care Act makes you realize even more how unnecessarily complicated this legislation had to be merely to accommodate the private insurance industry. If you are suffering from euphoria, read this rule and it will cure you.
As everyone knows, the Affordable Care Act was written by and for the private insurance industry. Just to show how much the insurance industry’s influence extends into the Obama administration you merely need to look at the rule on the governing board composition and conflict of interest, to wit, “representatives of health insurance issuers, agents, brokers, or other individuals licensed to sell health insurance may not constitute a majority of the governing board.”
Absolutely astounding! The private insurance industry can occupy up to one-half of the seats on the governing board! Amongst all of the other members of the board, they need only one friend. Watching the reform process take place it is clear that they have friends everywhere!
During the comment period, many expressed concern about this obvious conflict of interest, suggesting even that insurers participate as an advisory group rather than through board membership. And HHS’s response? “We believe that further definition of conflict of interest may create inconsistencies with State law and other existing State standards.”
This is an outrage! Mobilize the forces!
