By Thomas Lane
Minnesota Reformer, Aug. 11, 2025
When we hear about health policy changes in the news, usually the numbers we hear are related to insurance: How many people will become insured or uninsured as a result of the latest legislation? Analysts — and as a result, news reporters, too — tend to use these numbers because they’re relatively simple to predict and understand.
But at the end of the day, health insurance is just a little card legally linked to a thick stack of paperwork in some office somewhere. Insurance numbers don’t really tell us much about what we actually want to know, which is the human health impact. How many medically avoidable deaths will a given piece of legislation prevent or cause? How many will or won’t get the care they need? How many more will or won’t be in medical debt?
Congress passed and on July 4 President Trump signed his “One Big Beautiful Bill Act,” the largest ever cut to government health care funding in U.S. history. The Congressional Budget Office projects the law will push about 10 million Americans off of health insurance while growing the deficit by $3.4 trillion over the next decade.
Health economists have studied the link between health insurance and health outcomes and can estimate how many more preventable deaths Americans will suffer as health coverage declines, among other outcomes.
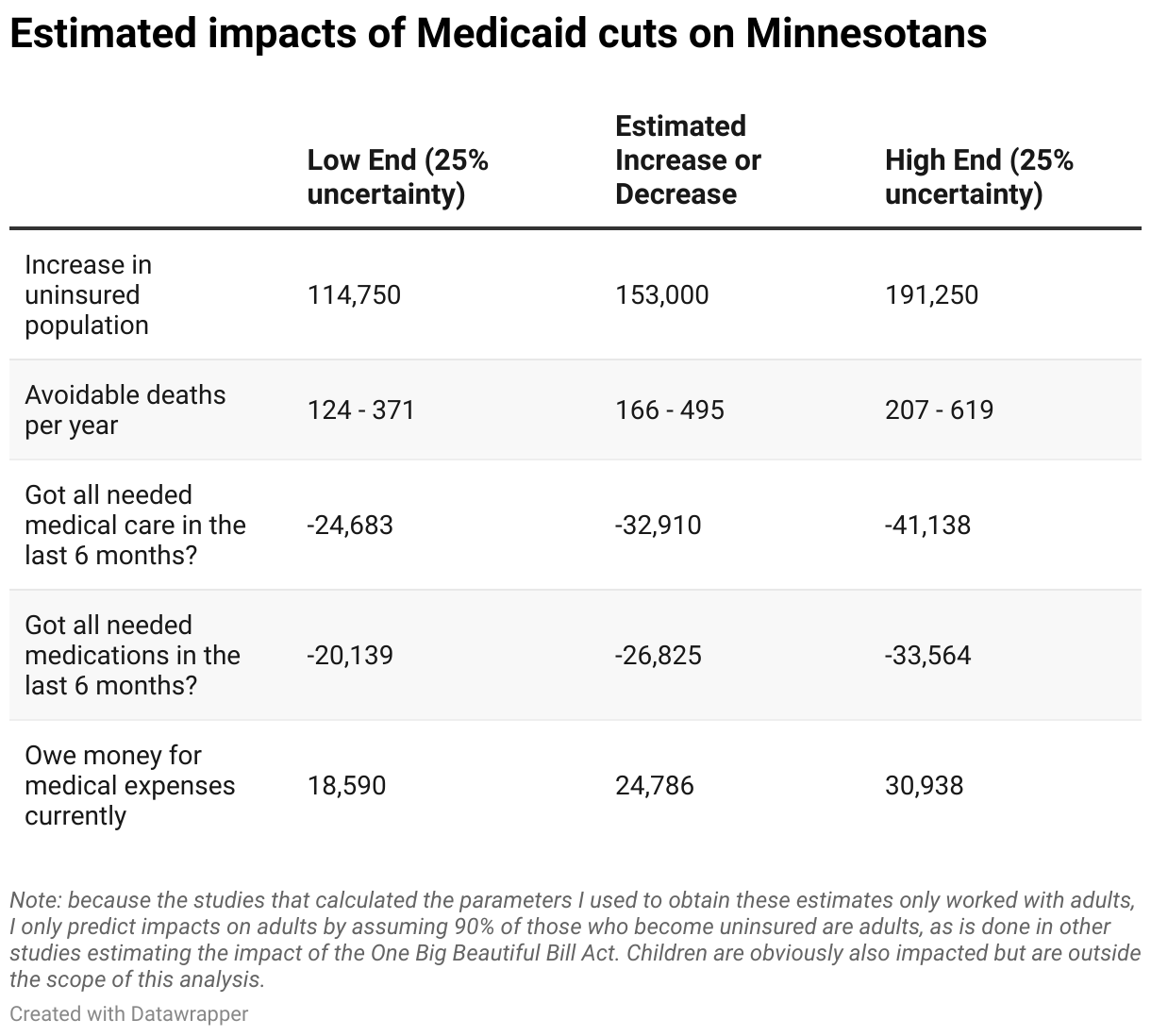
The Minnesota Department of Human Services recently released preliminary estimates that about 140,000 Minnesotans will lose their health insurance as a result of the legislation.
Additionally, due to upcoming subsidy expirations and rule changes for the Affordable Care Act’s insurance markets (“Obamacare”), health policy analysts at KFF have predicted an additional 5.1 million Americans will become uninsured nationwide, leading to an additional 13,000 uninsured Minnesotans.
Using this 153,000 figure, we can estimate that roughly one more Minnesotan will unnecessarily die per day as a result of losing coverage. Tens of thousands more will forego necessary care, miss medications, and rack up medical expenses they cannot afford.
Make no mistake, however. The craziest part of all of this should not be these figures themselves. It’s the fact that they can mostly still be prevented from coming to fruition by our state Legislature.
KFF estimates that the One Big Beautiful Bill Act is expected to cost the state up to $2.4 billion per year over the next decade, leaving a big hole for our state legislators to fill. Although some of these harms are caused by Congress’s imposition of work requirement paperwork burdens on Medicaid beneficiaries that the state cannot do much about, most of them come from the funding cuts, and funding cuts are something the state can definitely do something about. Minnesota just needs to come up with roughly $2.4 billion on its own.
How exactly can the state find such a large sum of money — roughly 6% of the state general fund budget? Believe it or not, it’s not actually that complicated. Currently, the state runs Medicaid through private third-party administrators called managed care organizations, or MCOs. These MCOs are a product of the 1990s, when the public policy world thought the problem with health care was that people were using too much of it, and health care needed gatekeepers.
It’s a rather evidence-free claim. Consider that Americans actually use less care than people in Europe and Canada despite spending far more per capita than them, all while also living shorter, less healthy lives. Nonetheless, the MCOs still run Minnesota’s Medicaid program, adding significant administrative expenses onto the state budget while doing nothing to make health care better.
Connecticut got rid of these wasteful MCO contractors in 2012, instead opting to run its Medicaid program itself. Unsurprisingly, they saved lots of money doing so. How much would Minnesota save if it spent per beneficiary what Connecticut does on Medicaid? About $1.5 billion annually, according to my analysis.
Given the $2.4 billion in cuts also includes some money cut from non-health care areas, that $1.5 billion in savings is likely enough to fill most of the health care-related hole in the state budget! With that money, the state can ensure tens of thousands of Minnesotans get the care they need while preventing closures of Minnesota hospitals and nursing homes that depend on Medicaid for funding.
During the last legislative session, I wrote a column in support of legislation called the Patient-Centered Care bill that would more or less copy what Connecticut did (SF1059/HF255). Unfortunately, neither the state House nor Senate brought it up for serious consideration.
Back then, it was admittedly still uncertain whether Congress would actually pass massive cuts to Medicaid, but it did, and now there are no more excuses. Our state Legislature can quite easily alleviate most of the financial problems Congress has passed onto it and thereby save lives.
All they have to do is pass a not very big but in my opinion quite beautiful bill to cut wasteful MCO middlemen out of our Medicaid program.

