Title: Yes, We Can Have Improved Medicare for All
Year: 2019
Author: Gerald Friedman
Institution: University of Massachusetts at Amherst
Funding Source: Hopbrook Institute
Plan Analyzed: H.R. 676
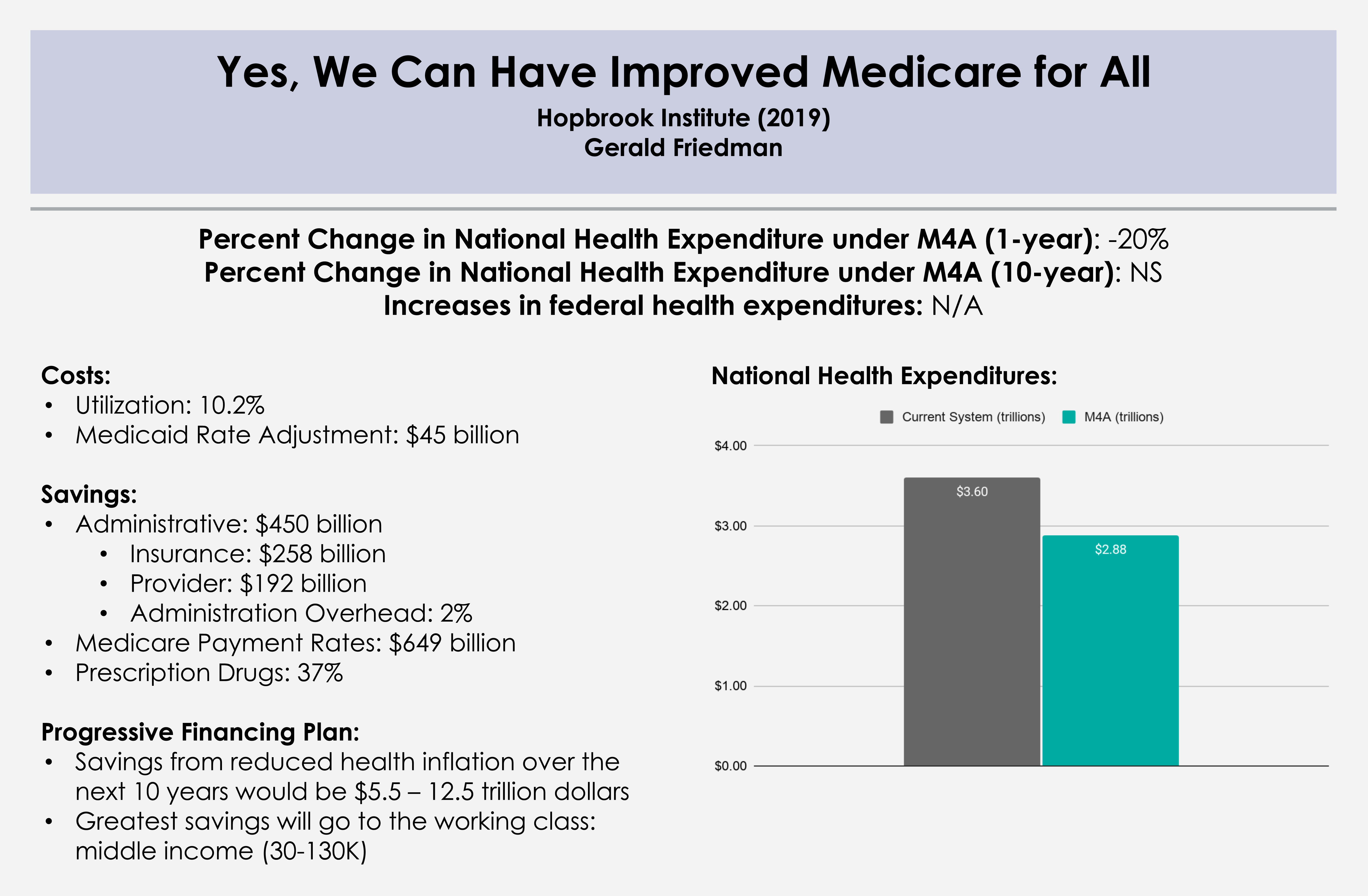
Percent Change in National Health Expenditure under M4A (1-year): -20.0% (2019)
Percent Change in National Health Expenditure under M4A (10-year): -20.6% (2019-28)
Read Study:
Yes, We Can Have Improved Medicare for All
Abstract:
Growing public support for universal health coverage through a public program has provoked increasing attention to the question of how to finance such a program. There should not be any controversy about our ability to pay for universal health care. Given the nearly universal agreement that the current health-care system involves administrative waste and monopoly pricing, a system that would be more efficient and would reduce both should certainly be affordable. Studies finding higher costs for universal coverage programs have reached their conclusions by acknowledging efficiency savings but dismissing them by emphasizing, even exaggerating, the higher costs of providing better access to health care. Such studies provide a poor guide to the possibilities for an overhaul of our health-care finance system. In this paper, I discuss the financing of a universal health-care program, beginning with a discussion of current projected spending and the savings to be achieved through administrative efficiency and reducing monopoly pricing. Next, I outline increased spending associated with universal coverage through covering the uninsured and reducing barriers to access. I consider the net cost of universal coverage, after taking account of savings and the cost of extending and improving coverage, under various scenarios with alternative immediate savings and savings over time. Finally, I discuss sources of funding for such a program, beginning with public funds already committed and including possible additional sources of revenue. I develop funding plans under a variety of assumptions regarding the course of the single-payer system, and under alternative assumptions regarding revenue sources. This work shows that compared with the current system of health-care finance, a program of Improved Medicare for All could save Americans over $1 trillion in the first year, and savings could increase over time. Because some of the savings would be returned to health care through programs of universal coverage and improved access, net savings could be over $700 billion in the first year, rising over the next decade. Depending on the assumptions made and the program details, total financial savings, after taking account of program improvements, would come to $10 trillion or more over the next decade, on top of gains in quality of life and reduced mortality through universal access. A variety of models are compared, with varying assumptions of the magnitude of administrative savings and savings through reduced monopoly rents, as well as savings from bending the cost curve and maintaining some cost-sharing. Overall, the ten-year national savings on health-care expenditures range from a low of over $6 trillion to a high of over $13 trillion. In every model tested, Improved Medicare for All is cheaper than the current system even while providing improved health care.
Overview:
Comprehensive cost analysis conducted by Gerald Friedman updating his previous work on the subject with similar considerations for financing options.
- Section 1: Current spending and waste
- Administrative savings in provider offices
- Savings from pricing at Medicare negotiated rates
- Drugs and medical devices
- Hospital and physician practices
- Section 2: Additional spending with universal coverage
- Medicare premiums
- Cost of universal coverage
- Cost of eliminating barriers to access
- Section 3: Total Spending with Medicare for All
- Section 4: Paying for Medicare for All
- Available revenues
- New revenues
- Conclusion: We can afford Improved Medicare for All