By Joan Alker
Georgetown University Health Policy Institute, November 28, 2018
For the past eight years, CCF has published a report tracking health coverage rates for children across the country. This year, for the first time since we began writing this report, the number and rate of uninsured children in the United States went up.
For many years, that rate has been declining thanks to bipartisan efforts to extend coverage through Medicaid and the Children’s Health Insurance Program (CHIP). But in 2017, approximately 276,000 more children became uninsured, leading to a total of 3.9 million uninsured children nationwide. The rate for children age 18 and under went up from 4.7 percent in 2016 to 5 percent in 2017, according to our analysis of U.S. Census Bureau’s American Community Survey data.
While this may not seem like a huge change, both of these increases are unprecedented in the past decade. Even more troubling, the number of uninsured children increased during a time of economic strength – in fact, at a time when one would expect the uninsured rate to go down, as more children were covered by employer-sponsored insurance in 2017.
However, coverage for children from public sources, Medicaid and CHIP, and in the individual market – inside and outside the Marketplace – decreased during this time period. That caused the number of uninsured children to go up – despite the strong economy.
I’ve written this report for eight years in a row now, and I found it even more notable that no state, except for the District of Columbia, saw any measurable progress in reducing the number of uninsured children in 2017. Never before have we seen such uniformity in state behavior. This finding underscores that even states with the best of intentions were not able to overcome the negative national currents that are affecting children’s health coverage.
Why do we think this is happening? We can’t know for sure, but here are some of our best guesses:
The majority of uninsured children are already eligible for Medicaid or CHIP but are not currently enrolled. The name of the game here is to make sure that families are aware that their child has a path to coverage and that these kids get enrolled and stay enrolled. For these families, 2017 was a year of constant news about the President and Congress wanting to take coverage away – first with the attempt to repeal the Affordable Care Act and make drastic cuts to Medicaid, all of which continued with a last gasp effort in September 2017.
Then on September 30, funding for CHIP expired and, in an unprecedented delay, Congress did not extend funding until early 2018 – again with families hearing that their state might have to close its CHIP program. At the same time, the Trump Administration began efforts to sabotage the ACA’s Marketplace including cuts to advertising, outreach and enrollment funding for navigators – who were playing an important role connecting families with public coverage, with the repeal efforts raising insurer uncertainty and driving up premiums.
The Trump Administration also began a series of actions hostile toward immigrant families. One quarter of children living in the United States has a parent who is an immigrant. For these “mixed status” families, there is likely a heightened fear of interacting with the government and this may be deterring them from signing their eligible children up for government sponsored health coverage.
As a result, the “welcome mat” for coverage has been pulled back and we see the results – more uninsured children.
With an improving economy and low unemployment rate, the fact that our nation is going backwards on children’s health coverage is very troubling. Without serious efforts to get back on track, the decline in coverage is likely to continue in 2018 and may in fact get worse for America’s children.
Joan Alker is the Executive Director of the Center for Children and Families and a Research Professor at the Georgetown McCourt School of Public Policy.
Comment:
By Don McCanne, M.D.
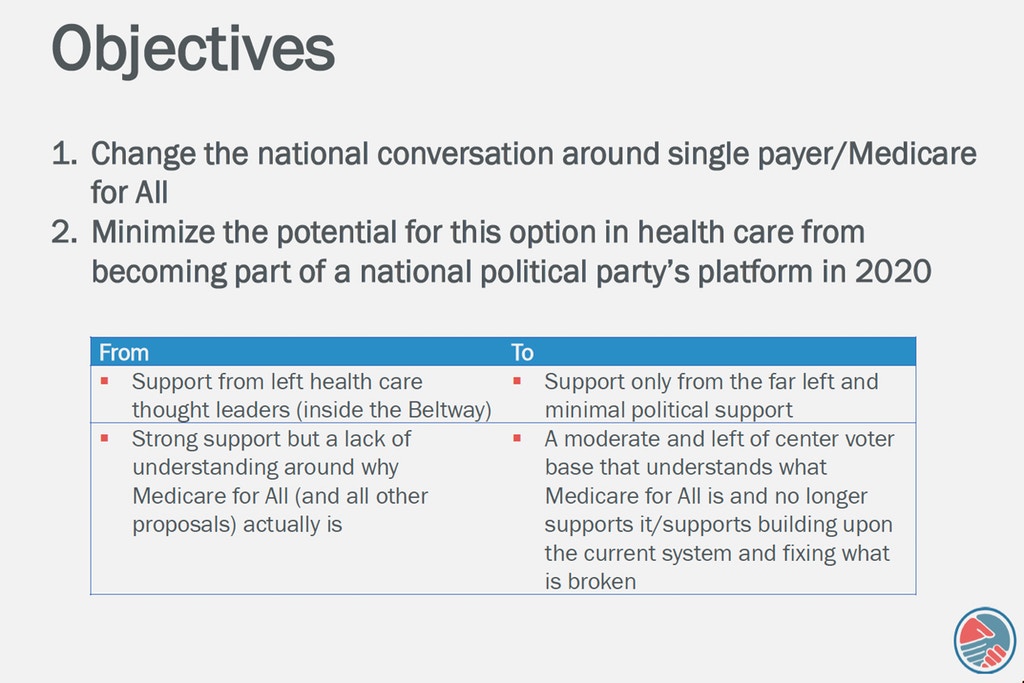
Imagine if everyone were automatically enrolled in a national health program for life. No resident would be uninsured. We could do this if we enacted and implemented a Single Payer Medicare for All program. Yet, because we insist on perpetuating our unstable, unsatisfactory system of financing health care, we are leaving almost 4 million children without any insurance coverage at all. Our health policy decisions border on the criminal.
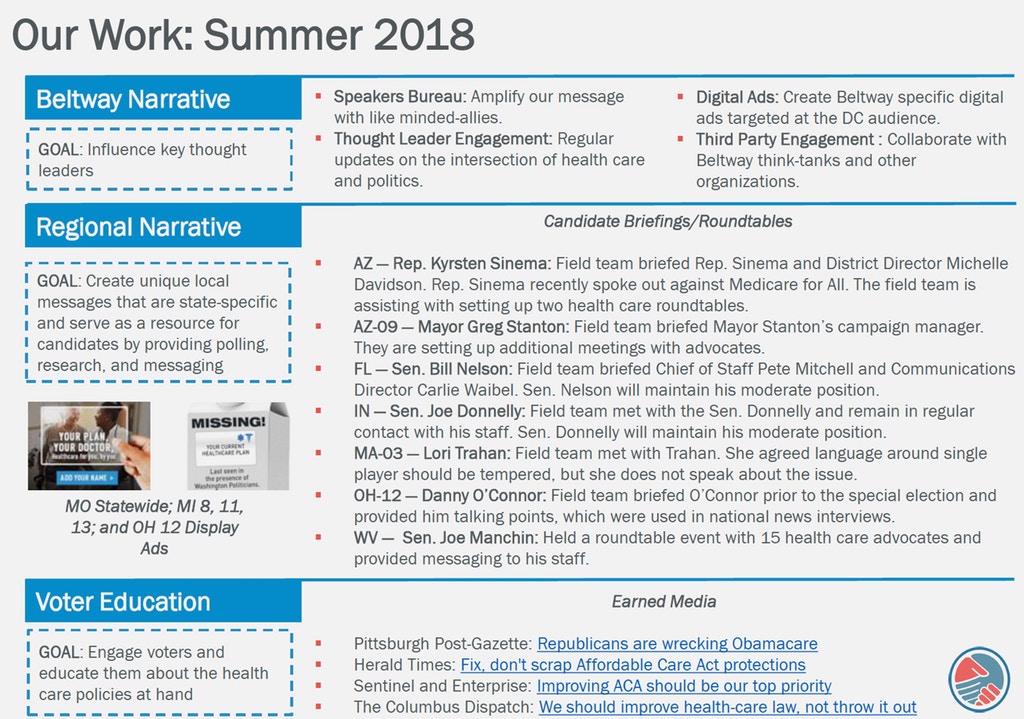
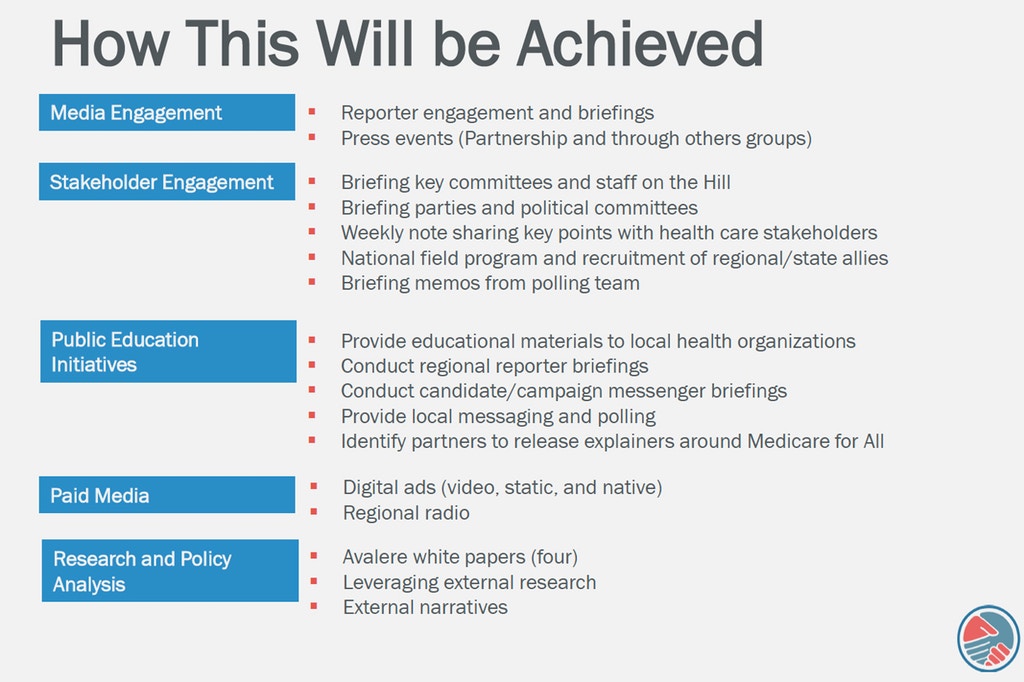
Medicare for All has become a very popular concept and was used in the recent election to secure votes for proponents of reform. Yet before the next session of Congress has even begun, we are already seeing widespread efforts to suppress talk of Medicare for All and instead to support mere tweaks to our current grossly inadequate model, though some would cut coverage back even further.
Suppose Congress were to pass an alternative proposal such as a public option Medicare for Some, will all of those 4 million children be automatically enrolled? Of course not. By merely tweaking our current dysfunctional system we will perpetuate a large unnamed category of the uninsured. Perhaps we should label this group, “No Medicare for Them.” Those supporting deficient proposals should be the ones to explain to these uninsured children and their parents why, in a democracy, we support health financing policies that leave them out. In fact, someone needs to explain it to me. Why do we?
Stay informed! Visit www.pnhp.org/qotd to sign up for daily email updates.