The Case Against Privatization of U. S. Health Care
2018 Annual Meeting Materials

The Medicare for All Act of 2019

Recruit Colleagues
The official blog of PNHP

2020 Virtual Annual Meeting
2018 SNaHP Summit Materials
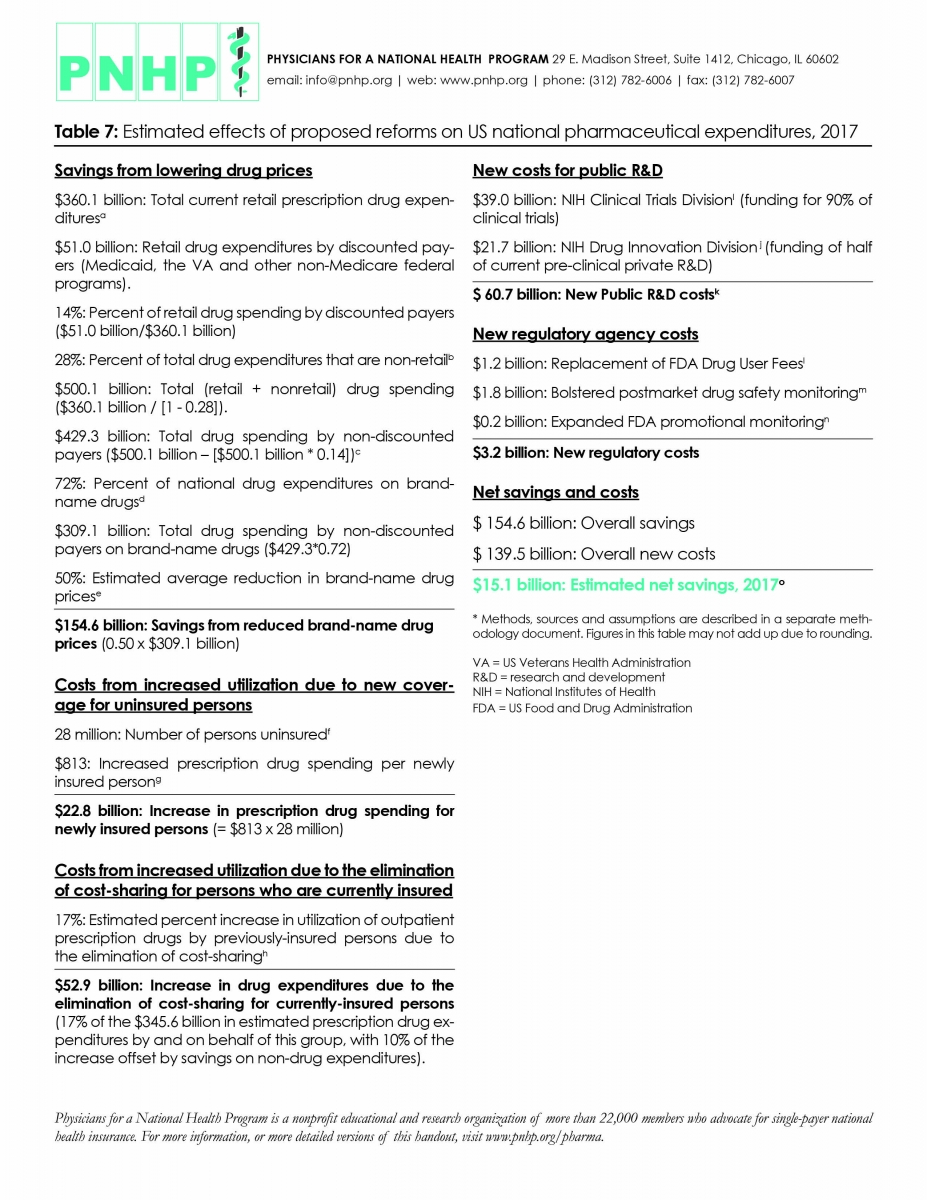
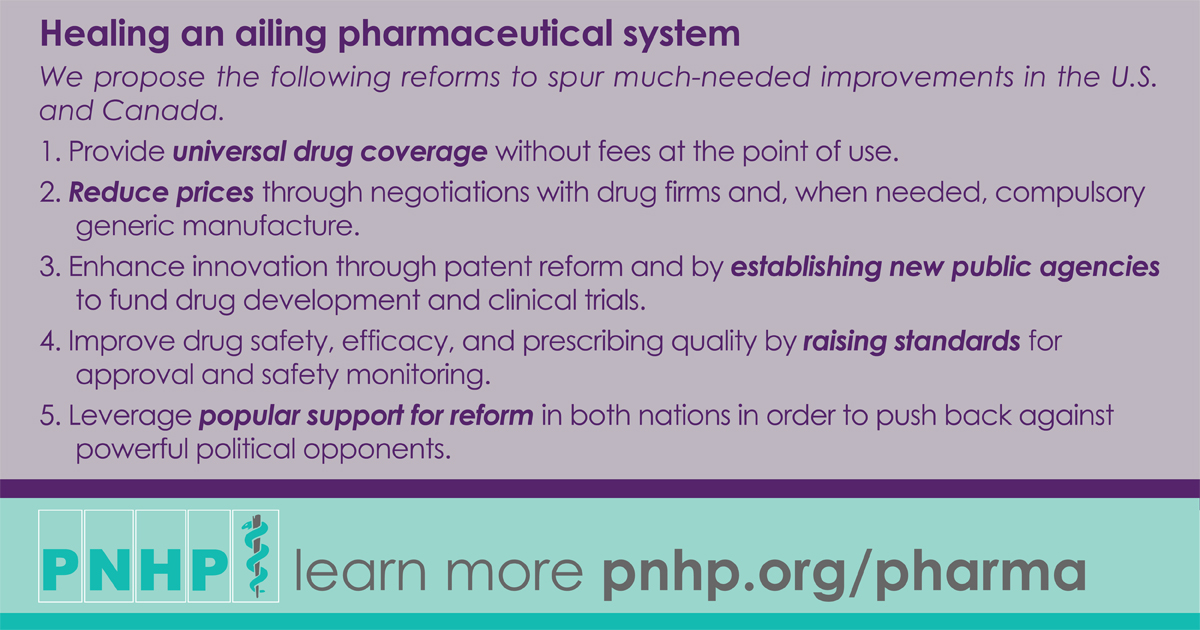
Healing an ailing pharmaceutical system: economic analysis and supplemental materials
Healing an ailing pharmaceutical system highlights the need for fundamental reform
PNHP pharma reform proposal in the news
2016 Annual Meeting Materials

PNHP leaders join Sen. Sanders in Canada