PNHP is committed to focusing on specific “Kitchen Table” issues, to show how single-payer Medicare for All would address Americans’ most pressing health care problems. See below for materials related to our Spring 2021 issue, mental health care, and scroll to the bottom for a list of additional topics.
Mental health care (Spring 2021)
The United States was facing a mental health crisis before COVID-19, but the pandemic has made these long-standing problems considerably worse. Commercial health insurance has no interest in addressing this crisis. When it comes to mental health care, we need improved Medicare for All.
We encourage you to share the materials below with your colleagues, family members, friends, and neighbors during the spring of 2021 to remind them that mental health care is a kitchen table issue…and that Medicare for All is a necessary part of the solution.
Complete mental health care toolkit
- One-page talking points handout: Medicare for All means Mental Health Care for All
- Comparison chart: Barriers to mental health care — Commercial insurance v. Medicare for All
- Problems and Solutions: How Medicare for All would improve mental health care
- PNHP Policy Primer: America’s mental health care crisis and Medicare for All
- PowerPoint slides: Medicare for All means mental health care for all (also available HERE as a Keynote and Google Slides compatible deck)
- Webinar: Chris Cai on mental health care for all
- Podcast: Dr. Claire Cohen on meeting the mental health needs of children and adolescents
- Podcast: Dr. Leslie Gise on how our current “system” fails people with mental health conditions
- Media outreach: Sample letters to the editor
- Video: Mental health professionals speak out on Medicare for All
- Video: Navigating the mental health care maze
- Social media: Share on Facebook, Twitter, or Instagram
Webinar: Chris Cai on mental health care for all
Video: Mental health professionals speak out
Video: Navigating the mental health care maze
If you need assistance with events or actions, contact the PNHP organizing team at organizer@pnhp.org. For help with messaging materials, contact PNHP communications specialist Clare Fauke at clare@pnhp.org.
If you would like to provide expertise or help develop materials for future Kitchen Table topics, please contact PNHP president Dr. Susan Rogers at s.rogers@pnhp.org.
Additional topics
Review previous installments of the Kitchen Table Campaign, and stay tuned for additional topics in the future:
- Surprise billing (January 2020)
- Racial health inequities (February 2020)
- Rural health (March 2020)
- Pandemics and public health emergencies (April 2020)
- COVID-19 and racial health inequities (Spring 2020)
- COVID-19 endangers health care workers (Summer 2020)
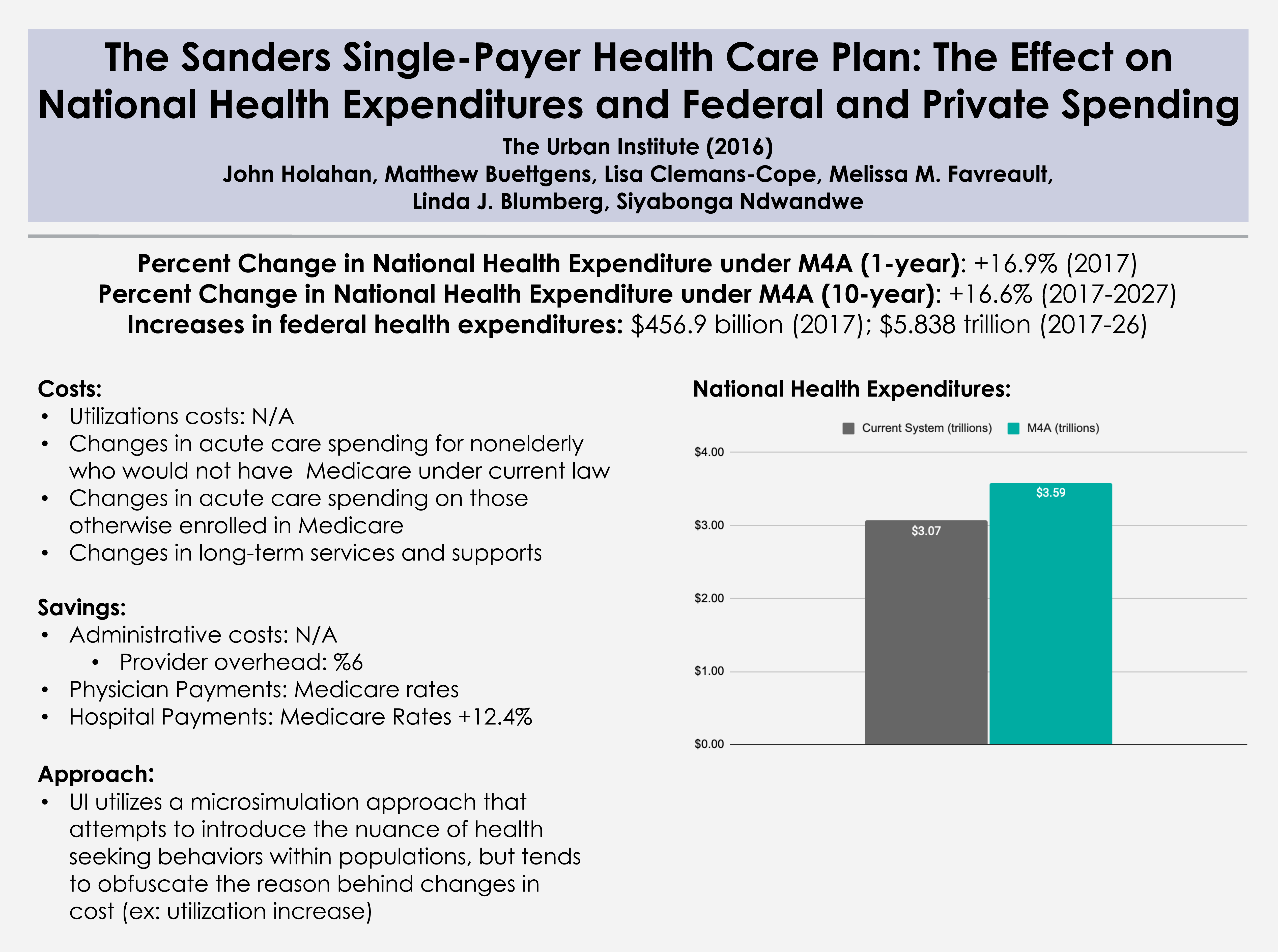
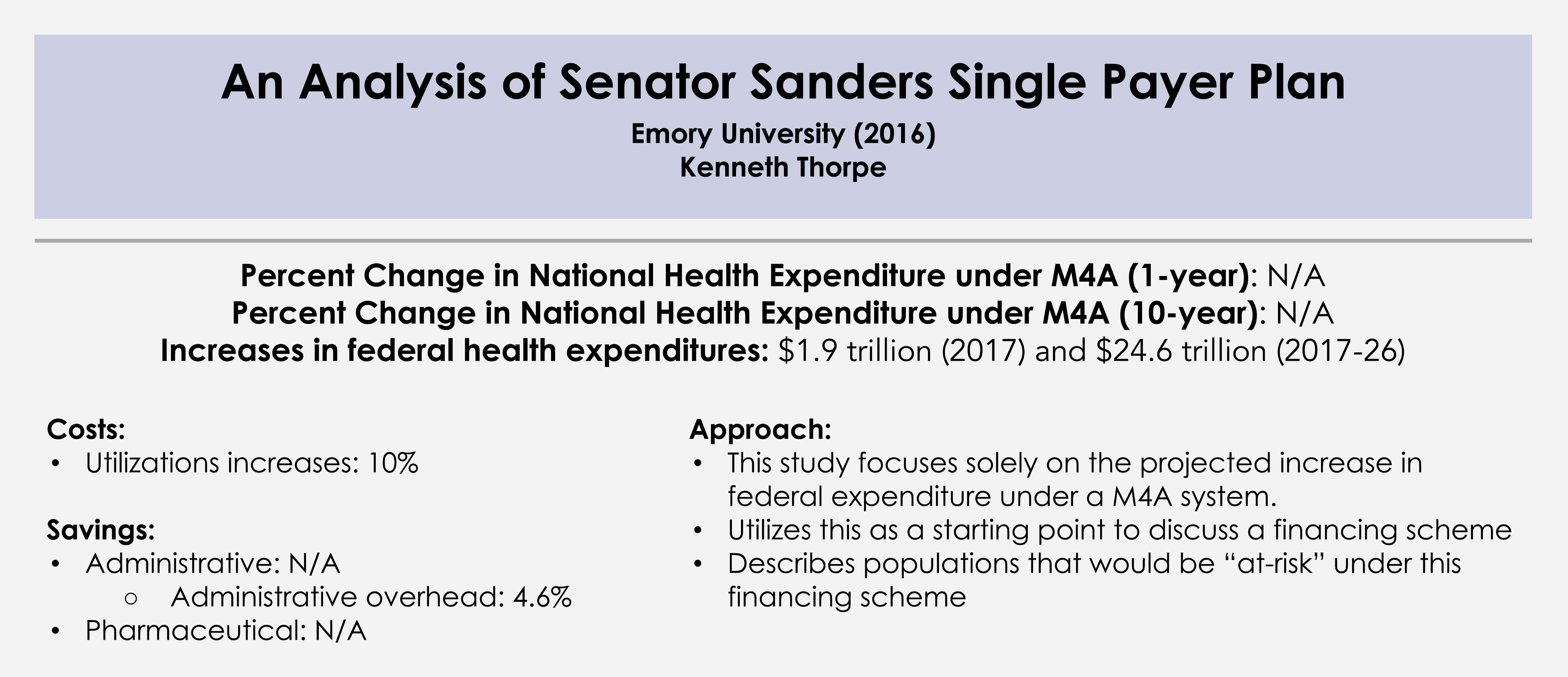
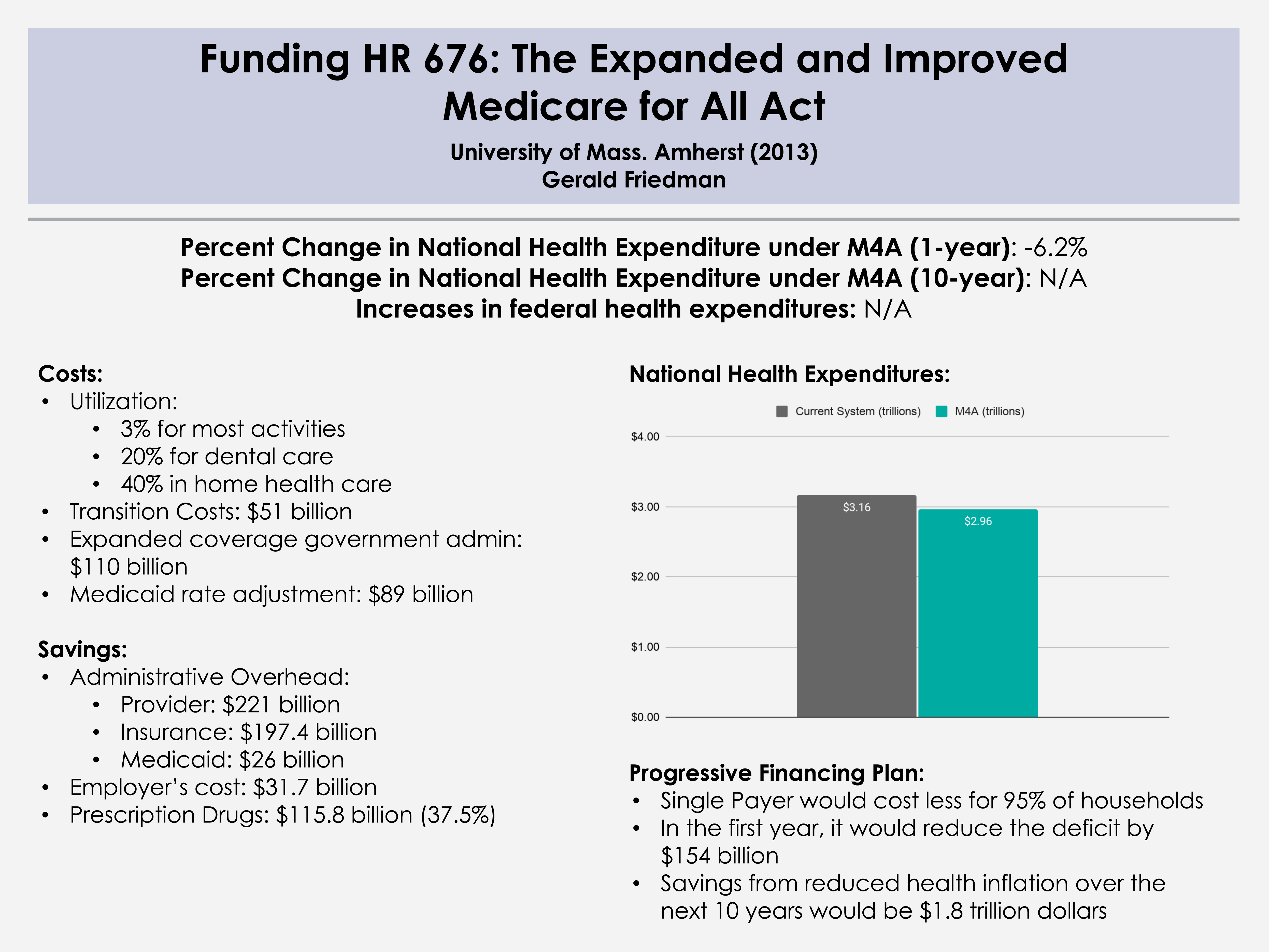
- Measuring candidate health plans (Fall 2020)
- Mental health care (Spring 2021)







{kind=link}