Sen. Bernie Sanders (I-Vt.) has introduced substantive single-payer legislation in the U.S. Senate. The Medicare for All Act (S.4204), which was filed May 12, 2022, would establish a publicly-funded national health program that would guarantee comprehensive, high-quality care for all residents of the United States.
full legislative text:
https://www.congress.gov…
PNHP analysis:
https://pnhp.org…
Sen. Sanders press release:
https://www.sanders.senate.gov…
U.S. Senate hearing | Medicare for All: Protecting Health, Saving Lives, Saving Money:
https://www.budget.senate.gov…
Overview of the bill
Based on our analysis, we find the Medicare For All Act of 2022 to be a significant step forward in the fight for single payer. Taken together with Rep. Pramila Jayapal’s Medicare for All Act (H.R. 1976), it would transform U.S. health care from a market commodity into a full-fledged human right.
What’s different in this year’s version?
The 2022 bill includes some major improvements from the 2019 version, bringing it closer to PNHP’s gold standard as established by the Physicians Proposal.
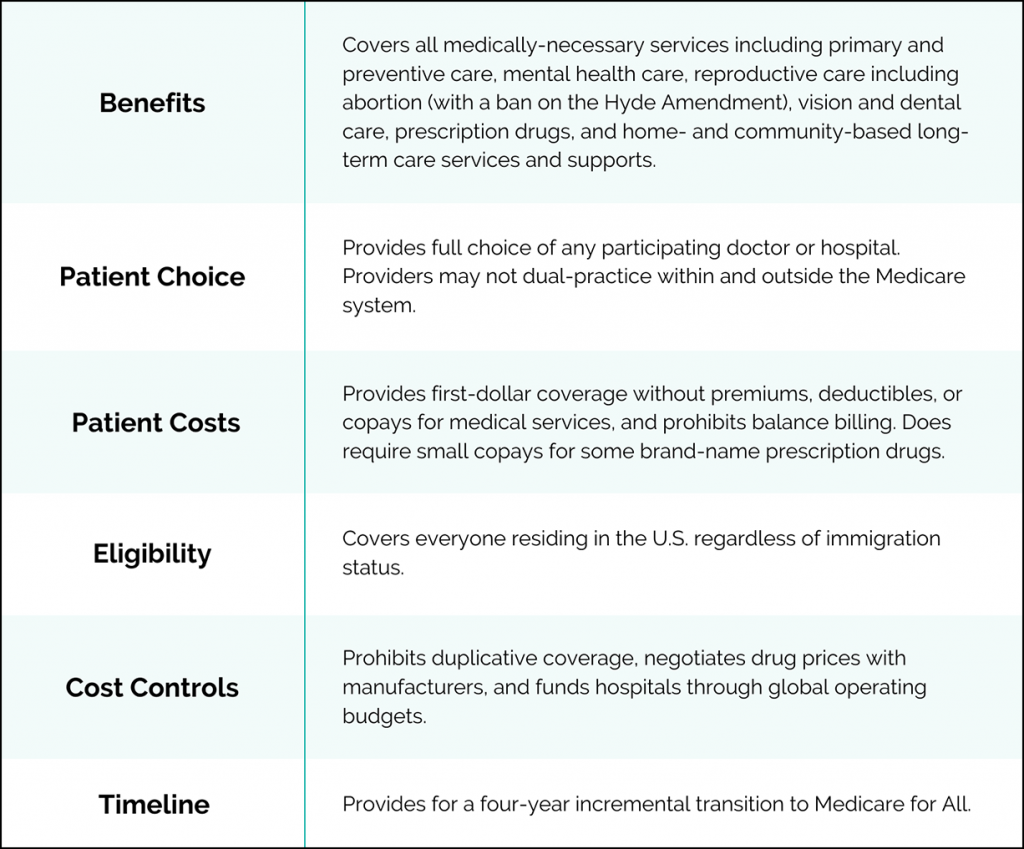
- Global budgeting of hospitals and other institutional providers: Global budgets would fund hospitals with annual lump sum payments which can be used for patient care — not for profits, advertising, or executive bonuses — with separate funding for capital projects. PNHP estimates that global budgets would save $220 billion per year; they would also prevent hospital closures by providing facilities in rural and other underserved communities with stable funding, which can be quickly supplemented during public health emergencies. Global budgets also promote health equity by funding services and capital projects based on community health needs (i.e., mental health, obstetrics, and HIV care), not what’s most profitable for hospitals (i.e., elective surgeries).
- Standardized fee-for-service payments to providers: Establishes a national fee-for-service schedule for individual and group providers, similar to language in the House bill (H.R. 1976).
- Expanded benefits: Provides transportation for seniors with functional limitations, and expands mental health care by covering licensed marriage and family therapist and licensed mental health counselor services.
- Office of Health Equity: Establishes an Office of Health Equity to monitor and eliminate health disparities, and to promote primary care.
How can the bill be improved?
In order to realize the best possible vision for single payer, PNHP recommends several improvements to the Medicare for All Act that would save even more money and improve patient care:
- Cover all long-term care (LTC): While community-based LTC supports would be covered by Medicare for All, institutional LTC remains within Medicaid, preserving the state-based variations that contribute to inequities, injustice, and complexity. PNHP recommends moving all LTC services into Medicare for All.
- Shorten transition period: The four-year transition period gradually expands Medicare’s benefits and lowers the eligibility age, along with a “buy in” scheme that includes commercial Medicare Advantage plans. The transition period is needlessly complex, delays access to care for the most vulnerable patients, and could exacerbate inequalities. PNHP recommends a one-year transition.
- Eliminate prescription drug costs and strengthen price negotiations: While drug co-pays are lower than they were in the 2019 bill, even modest cost-sharing is a proven barrier to care. PNHP recommends eliminating all patient cost-sharing. While the bill does authorize Medicare to negotiate drug prices, it lacks certain safeguards if negotiations fail, such as direct procurement of drugs. PNHP recommends competitive drug licensing, direct procurement of drugs, and other safeguards if price negotiations fail.
- Ban (and buyout) investor-owned health facilities: This bill does not explicitly ban for-profit health facilities and agencies, which provide lower-quality care at higher costs than nonprofits. PNHP recommends an orderly conversion of investor-owned, for-profit providers to not-for-profit status.
Building momentum for single payer
See below for a list of current Medicare for All Act co-sponsors. It is important to build as much support for single payer as possible, and you can help!
- If your senators have already co-sponsored the Medicare for All Act, call and email to thank them. Also, ask them to help improve the bill by covering institutional long-term care, shortening the transition period, converting investor-owned health facilities to nonprofit status, and fully eliminating copays.
- If your senators have not co-sponsored the Medicare for All Act, call and email to encourage them to co-sponsor.
To find your senators by state, click HERE. If you have trouble locating contact information for your senators, call the U.S. Capitol switchboard at (202) 224-3121.
Current co-sponsors:
- Bernie Sanders (VT), lead sponsor – contact info
- Tammy Baldwin (WI) – contact info
- Richard Blumenthal (CT) – contact info
- Cory Booker (NJ) – contact info
- Kirsten Gillibrand (NY) – contact info
- Martin Heinrich (NM) – contact info
- Mazie Hirono (HI) – contact info
- Patrick Leahy (VT) – contact info
- Ben Ray Lujan (NM) – contact info
- Alex Padilla (CA) – contact info
- Edward Markey (MA) – contact info
- Jeff Merkley (OR) – contact info
- Brian Schatz (HI) – contact info
- Elizabeth Warren (MA) – contact info
- Sheldon Whitehouse (RI) – contact info
Senate Budget Committee hearing
On May 12, 2022, Sen. Sanders convened a U.S. Senate Budget Committee hearing, “Medicare for All: Protecting Health, Saving Lives, Saving Money.”
PNHP immediate past president Dr. Adam Gaffney testified alongside PNHP 2019 Annual Meeting keynote speaker Dr. Abdul El-Sayed and National Nurses United executive director Bonnie Castillo.
PNHP live-tweeted the hearing HERE.
Sen. Sanders on Fox News: “It’s time for Medicare for All”
Also on May 12, 2022, Sen. Sanders published an op-ed on the Fox News website making the case for single payer.
“The United States has the most dysfunctional, inefficient, bureaucratic and expensive health care system in the world,” he wrote. “That’s not just what I believe. That’s what the American people know to be true. According to a March 2022 survey by Gallup and West Health, an estimated 93 percent of American adults feel what they pay for health care is not worth the cost.” …
“Now is the time for Congress to stand with the American people and take on the powerful special interests that dominate health care in the United States. Now is the time to improve and extend Medicare to everyone.”