Physicians for a National Health Program (PNHP) is partnering with the Robert Wood Johnson Foundation (RWJF) to study the impact of financialization on U.S. health care. We are engaging with current health care professionals to better understand moral injury and distress, how these issues impact racial inequities in health care, and how best to remedy this worsening problem.
See our initial survey findings
Stay engaged with our moral injury work
What is “moral injury?”
As health care has been transformed from an essential service to a profit-driven business, the morale of the entire workforce—including physicians, nurses, and allied health professionals—has suffered. This trend has led to shortages as professionals are retiring early, cutting back work hours, quitting clinical medicine, and tragically committing suicide in increasing numbers.
These responses have often been misdiagnosed as “burnout,” but the lack of efficacy of standard treatments for burnout has led insightful scholars such as Drs. Wendy Dean and Simon Talbot to identify “moral injury” as a more accurate culprit.
Moral injury in health care is described as the challenge of knowing what care patients need, but being unable to provide it due to constraints beyond physicians’ control. As a result, the industry’s focus on burnout is insufficient and, in fact, causes harm by leading to a reliance on ineffectual “wellness” programs and an obscuring of root causes.
Without adequate data on moral injury, the ability of policymakers and stakeholders to address our health care crisis will remain limited.
Moral injury survey findings
In an effort to better understand moral injury in health care, PNHP surveyed workers throughout the medical profession and conducted a series of one-on-one interviews with currently practicing physicians. We gathered data points on the impact of financialization from our survey, and identified narratives from our interviews to more compellingly illustrate these data points. These elements will form the basis of our upcoming report, which will provide actionable recommendations for stakeholders.
Our survey of health professionals—including 1,126 currently practicing physicians—yielded striking results. We found that 87% of physicians reported at least mild burnout while 69% of physicians have left or considered leaving a position due to moral injury or distress.
For more information on our initial findings, see our one-pager HERE and watch our “Understanding Moral Injury in Medicine” webinar HERE.
Sharing our moral injury work
Our physician members—and everybody who is concerned about the financialization of health care—have a crucial role to play in sharing our moral injury findings.
PNHP national board member Dr. Toby Terwilliger provides some tips on sharing the survey above, but his advice also applies to sharing our moral injury project as a whole. Please reach out to your colleagues today, share our survey data and your personal experiences with moral distress, and continue the conversation about how to substantively address these issues.
Moral injury buttons

PNHP’s brand new buttons are perfect for wearing and/or distributing to health professionals in your network. Interested in sparking conversations about moral injury? Email rebecca@pnhp.org and we’ll happily send some buttons to you!
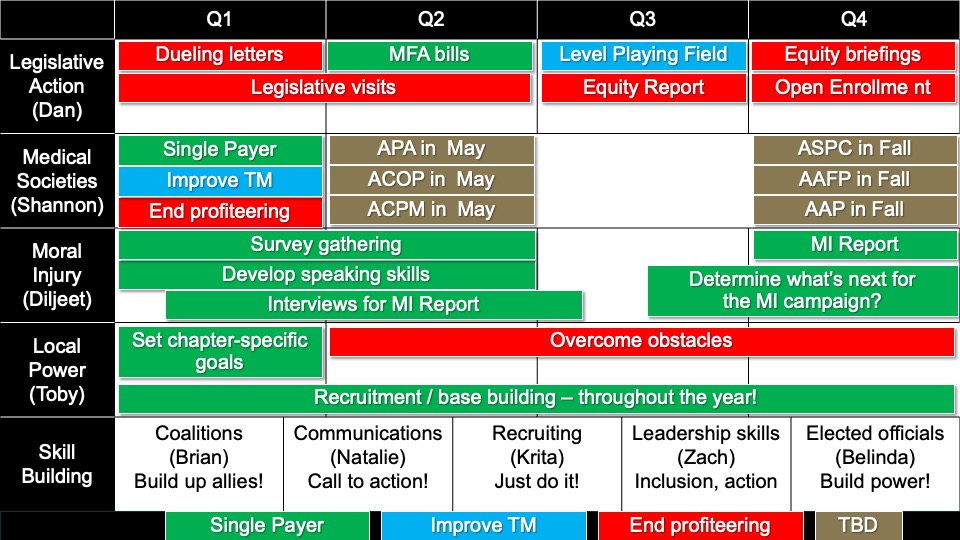
Learn more about our research process
PNHP president Dr. Diljeet Singh helped lead a workshop on moral injury at our 2024 Annual Meeting in Chicago, where she gave a detailed overview of the topic. You can download Dr. Singh’s slideshow HERE.
We’ve also developed a one-page info sheet with information about the project.
Respecting our participants’ privacy
PNHP’s moral injury survey covered delicate topics and gave participants the opportunity to share experiences from their practice—as well as experiences with specific employers, insurers, and other parties.
Rest assured that survey responses were anonymized through the use of unique ID numbers and that nobody outside of PNHP’s survey team will ever have access to individual replies.
We also asked survey respondents to share their email address, so we could follow up regarding potential 1:1 interviews. Please note:
- Individuals who were not already in PNHP’s database could opt in to receive updates about our moral injury project.
- If respondents were added to our email list, they could unsubscribe at any time (link at the bottom of all PNHP emails).
- PNHP will never sell or share emails collected through our moral injury survey.
Our project followed the rigorous practices of the Association for the Accreditation of Human Research Protection Programs (AAHRPP), and we obtained Institutional Review Board approval by the independent Pearl IRB, along with our consultant at Cambridge Health Alliance’s institutional IRB.
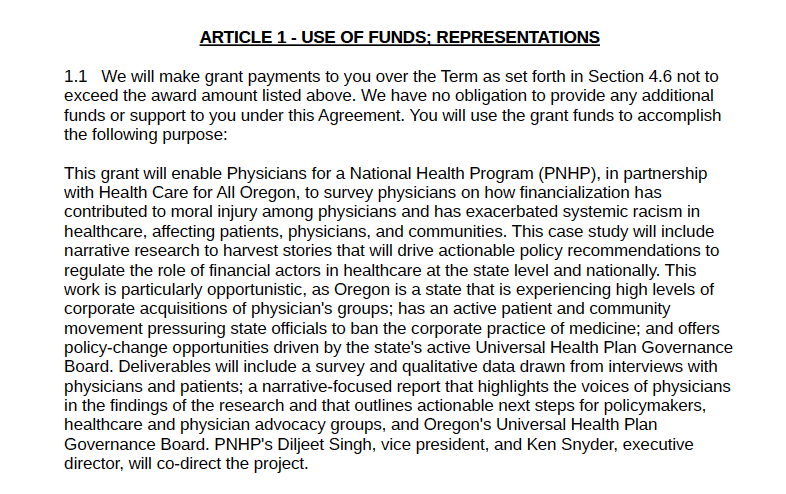
See the following documents for specifics on our survey, and the broader moral injury project:



 Matthew Petty
Matthew Petty Ananiya Asrat
Ananiya Asrat




 Dinner Keynote
Dinner Keynote


















 Keynote Speaker
Keynote Speaker Health Policy Update
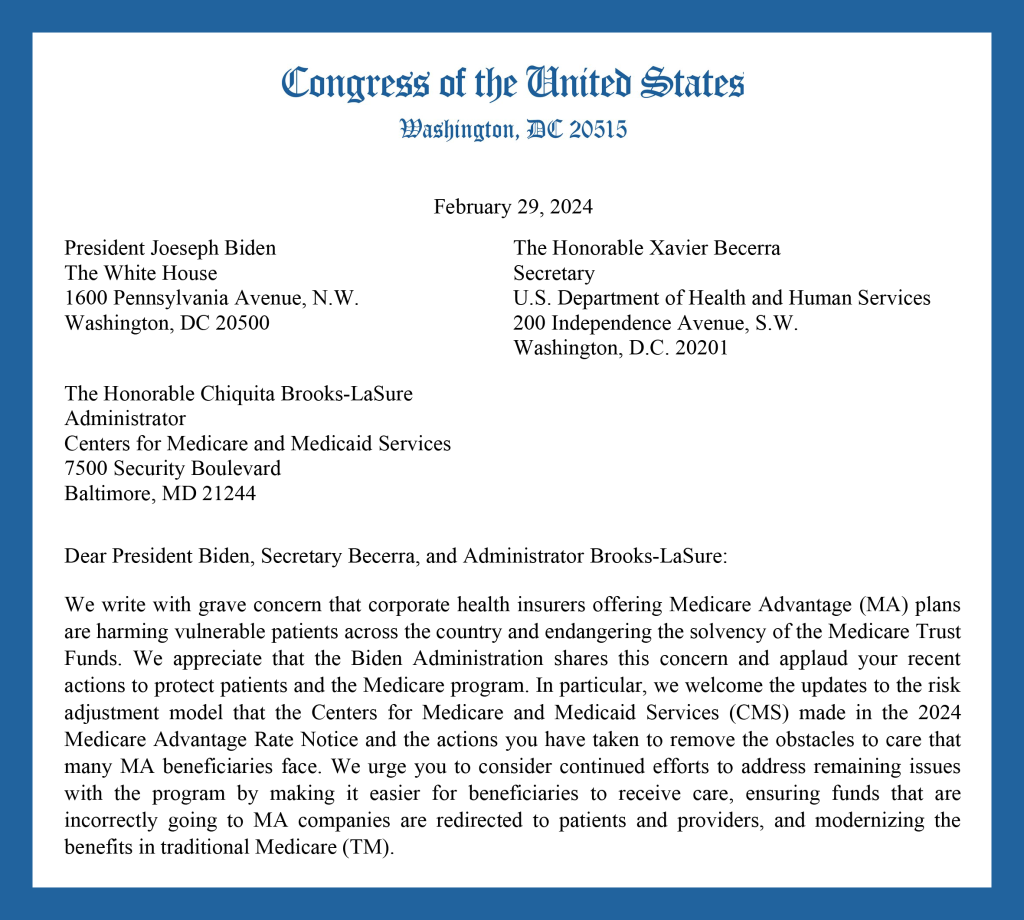
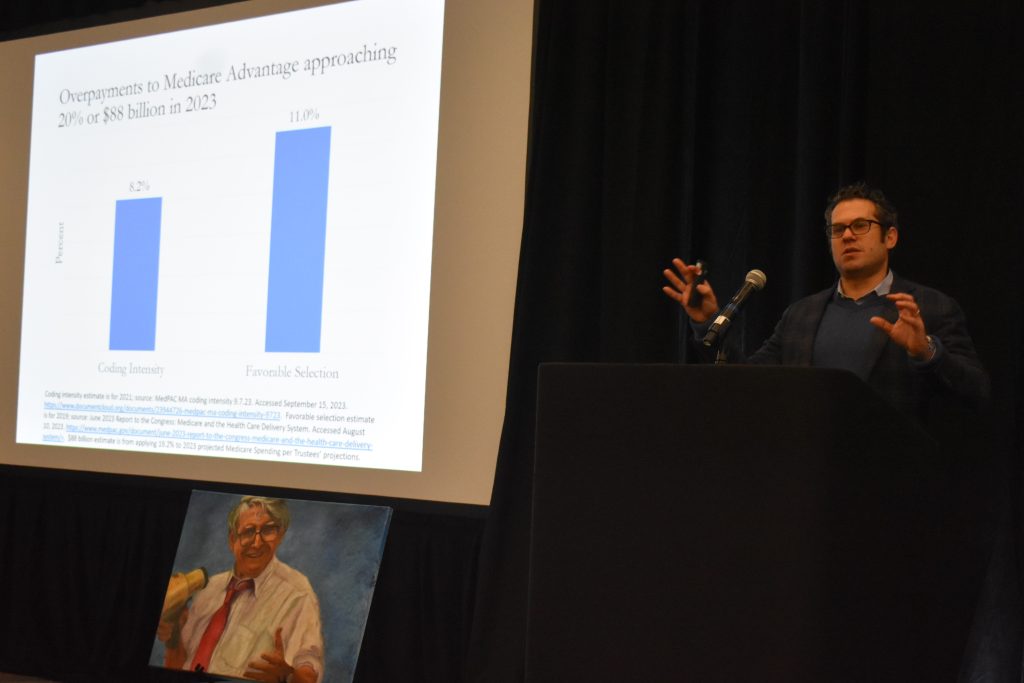
Health Policy Update Messaging Medicare Advantage
Messaging Medicare Advantage Building Progressive Power, Lessons from Georgia
Building Progressive Power, Lessons from Georgia



{kind=link}